Kara Atila, Akin Sakir, Dos Reis Miranda Dinis, Struijs Ard, Caliskan Kadir, van Thiel Robert J, Dubois Eric A, de Wilde Wouter, Zijlstra Felix, Gommers Diederik, Ince Can
Department of Intensive Care, Erasmus MC, University Medical Center Rotterdam, 's-Gravendijkwal 230, 3015 CE, Rotterdam, The Netherlands.
Department of Intensive Care, Hacettepe University Faculty of Medicine, Ankara, Turkey.
Crit Care. 2016 Oct 25;20(1):344. doi: 10.1186/s13054-016-1519-7.
Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) is an effective technique for providing emergency mechanical circulatory support for patients with cardiogenic shock. VA-ECMO enables a rapid restoration of global systemic organ perfusion, but it has not been found to always show a parallel improvement in the microcirculation. We hypothesized in this study that the response of the microcirculation to the initiation of VA-ECMO might identify patients with increased chances of intensive care unit (ICU) survival.
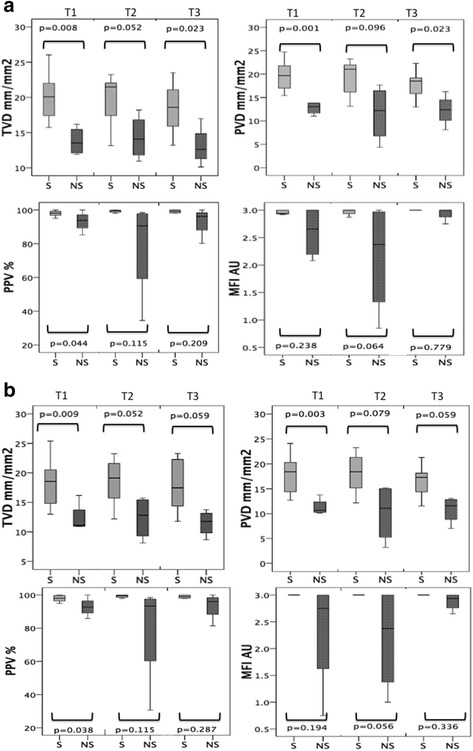
Twenty-four patients were included in this study. Sublingual microcirculation measurements were performed using the CytoCam-IDF (incident dark field) imaging device. Microcirculatory measurements were performed at baseline, after VA-ECMO insertion (T1), 48-72 h after initiation of VA-ECMO (T2), 5-6 days after (T3), 9-10 days after (T4), and within 24 h of VA-ECMO removal.
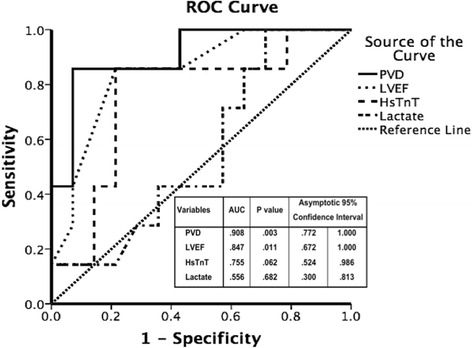
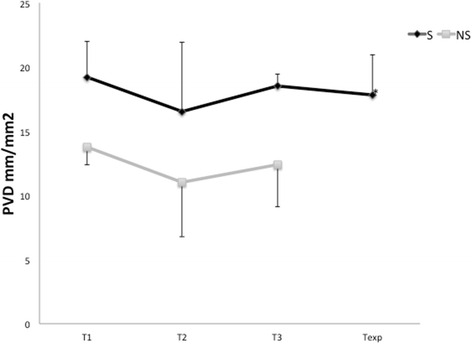
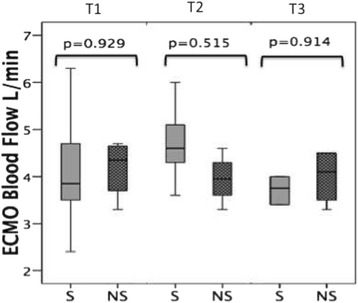
Of the 24 patients included in the study population, 15 survived and 9 died while on VA-ECMO. There was no significant difference between the systemic global hemodynamic variables at initiation of VA-ECMO between the survivors and non-survivors. There was, however, a significant difference in the microcirculatory parameters of both small and large vessels at all time points between the survivors and non-survivors. Perfused vessel density (PVD) at baseline (survivor versus non-survivor, 19.21 versus 13.78 mm/mm, p = 0.001) was able to predict ICU survival on initiation of VA-ECMO; the area under the receiver operating characteristic curve (ROC) was 0.908 (95 % confidence interval 0.772-1.0).
PVD of the sublingual microcirculation at initiation of VA-ECMO can be used to predict ICU mortality in patients with cardiogenic shock.
静脉-动脉体外膜肺氧合(VA-ECMO)是为心源性休克患者提供紧急机械循环支持的有效技术。VA-ECMO能使全身系统器官灌注迅速恢复,但尚未发现其总能使微循环得到同步改善。我们在本研究中假设,微循环对VA-ECMO启动的反应可能有助于识别在重症监护病房(ICU)存活几率增加的患者。
本研究纳入24例患者。使用CytoCam-IDF(入射暗场)成像设备进行舌下微循环测量。在基线、VA-ECMO置入后(T1)、VA-ECMO启动后48 - 72小时(T2)、5 - 6天后(T3)、9 - 10天后(T4)以及VA-ECMO撤除后24小时内进行微循环测量。
研究人群中的24例患者,15例存活,9例在接受VA-ECMO治疗期间死亡。存活者和非存活者在VA-ECMO启动时的全身整体血流动力学变量无显著差异。然而,存活者和非存活者在所有时间点的小血管和大血管微循环参数存在显著差异。基线时的灌注血管密度(PVD)(存活者与非存活者,19.21对13.78 mm/mm,p = 0.001)能够在VA-ECMO启动时预测ICU存活情况;受试者工作特征曲线(ROC)下面积为0.908(95%置信区间0.772 - 1.0)。
VA-ECMO启动时舌下微循环的PVD可用于预测心源性休克患者的ICU死亡率。