Veerus Piret, Fischer Krista, Hemminki Elina, Hovi Sirpa-Liisa, Hakama Matti
National Institute for Health Development, Tallinn, Estonia.
Estonian Genome Centre, University of Tartu, Tartu, Estonia.
BMJ Open. 2016 Oct 18;6(10):e011099. doi: 10.1136/bmjopen-2016-011099.
To analyse the effect of women's characteristics on their willingness to join a blind or a non-blind subtrial or to be excluded by physicians.
Primary prevention trial of postmenopausal hormone therapy (HT). A 2×2, randomised design with a non-blind HT arm or control arm and a blind HT arm or placebo arm.
3 clinical centres in Estonia.
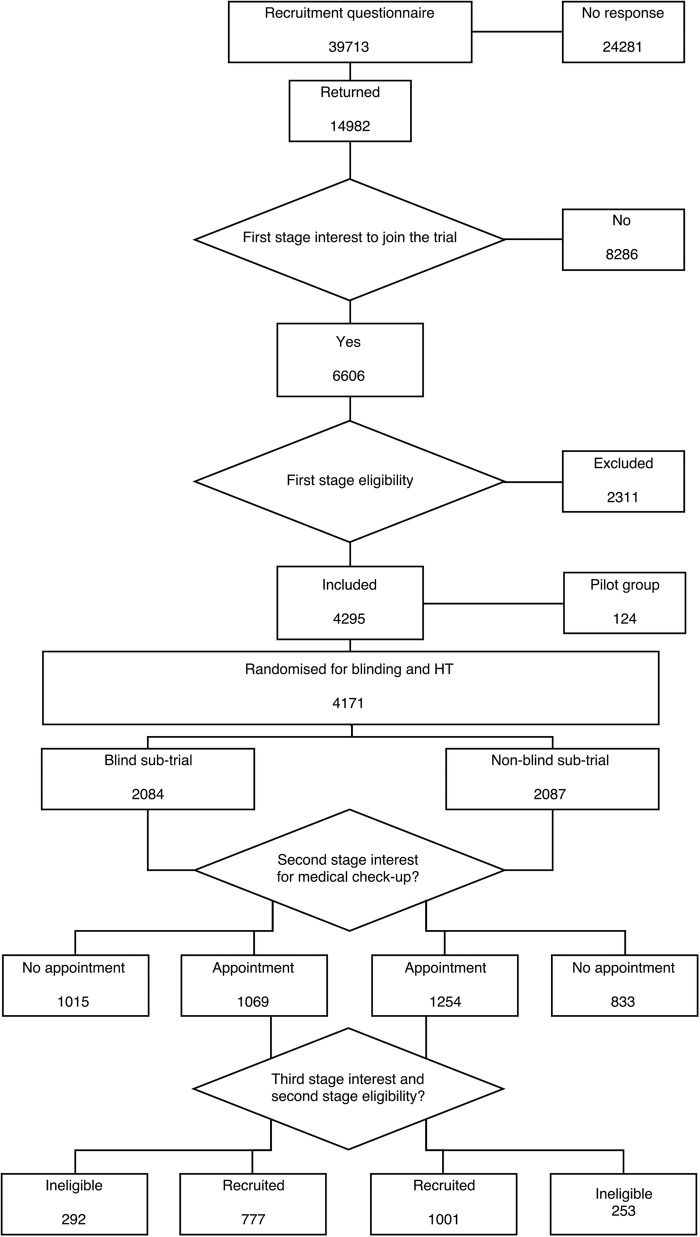
Interest in joining the trial was asked in a questionnaire together with demographic and health status data. Interested and eligible women were invited to a health examination that also informed whether they belonged to a blind or to a non-blind subtrial; the arm was not revealed. Trial physicians made further exclusions when checking the women's eligibility. Thereafter, informed consent was asked as detailed in the flow chart. Comparisons were made between non-blind and blind subtrials. Analyses were carried out for each of the background variables.
The proportion of willingness, eligibility and attendance.
Women randomised to the non-blind subtrial were more willing to join (relative risk (RR) 1.17) and more likely to be found eligible by physicians (RR 1.10) than women in the blind subtrial, resulting in larger attendance (RR 1.29). Women with higher education were differentially more willing to join the non-blind trial (RR 1.29) than those with basic education (RR 1.08); the differential willingness of never-smokers (RR 1.20) was larger than that of current smokers (RR 1.07). The differential exclusion by physicians by education and smoking were small. Some subjective symptoms (eg, diarrhoea/constipation, stomach pain) had reverse differential effects on attendance in the non-blind subtrial in comparison to the blind subtrial. Menopausal symptoms did not affect the differential interest, eligibility or attendance.
Blinding in RCT reduces attendance, due to decisions of the women and the trial physicians. Differential attendance by blinding may affect the generalisability of the results from trials.
ISRCTN35338757.
分析女性特征对其参与盲法或非盲法亚组试验意愿或被医生排除的影响。
绝经后激素治疗(HT)的一级预防试验。采用2×2随机设计,有一个非盲法HT组或对照组以及一个盲法HT组或安慰剂组。
爱沙尼亚的3个临床中心。
在问卷中询问参与试验的意愿以及人口统计学和健康状况数据。邀请感兴趣且符合条件的女性进行健康检查,同时告知她们属于盲法还是非盲法亚组试验,但不透露分组情况。试验医生在检查女性的合格性时进一步排除一些人。此后,按照流程图详细说明的那样获取知情同意。对非盲法和盲法亚组试验进行比较。对每个背景变量进行分析。
意愿、合格性和参与率。
随机分配到非盲法亚组试验的女性比盲法亚组试验的女性更愿意参与(相对风险(RR)1.17),并且医生更有可能认定她们合格(RR 1.10),导致参与率更高(RR 1.29)。受过高等教育的女性比接受基础教育的女性更倾向于参与非盲法试验(RR 1.29);从不吸烟者的差异意愿(RR 1.20)大于当前吸烟者(RR 1.07)。医生按教育程度和吸烟情况进行的差异排除较小。与盲法亚组试验相比,一些主观症状(如腹泻/便秘、胃痛)对非盲法亚组试验的参与率有相反的差异影响。绝经症状不影响差异意愿、合格性或参与率。
随机对照试验中的盲法会降低参与率,这是由女性和试验医生的决定导致的。因盲法导致的差异参与率可能会影响试验结果的普遍性。
ISRCTN35338757。