Department of Epidemiology, and Cardiovascular Surgery, The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Institute of Population Health Science, National Health Research Institutes, Zhunan, Taiwan.
Sci Rep. 2016 Nov 2;6:36482. doi: 10.1038/srep36482.
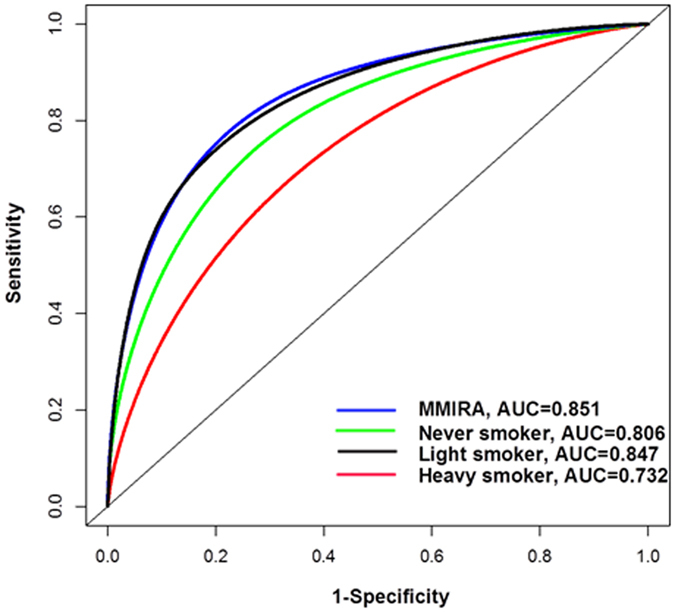
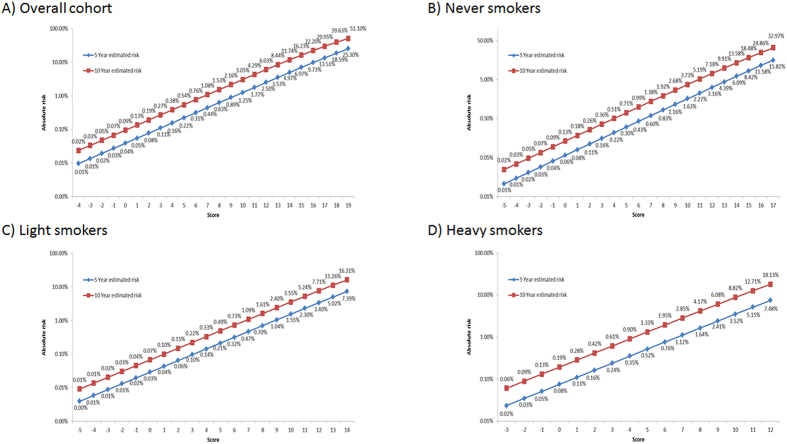
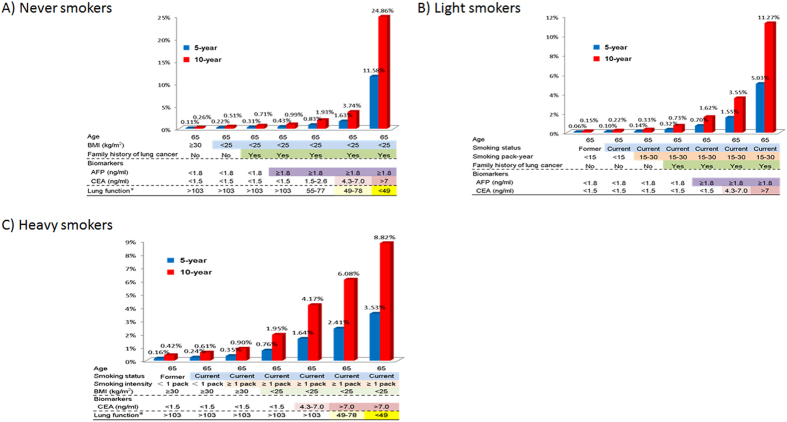
The objective of this study was to develop markedly improved risk prediction models for lung cancer using a prospective cohort of 395,875 participants in Taiwan. Discriminatory accuracy was measured by generation of receiver operator curves and estimation of area under the curve (AUC). In multivariate Cox regression analysis, age, gender, smoking pack-years, family history of lung cancer, personal cancer history, BMI, lung function test, and serum biomarkers such as carcinoembryonic antigen (CEA), bilirubin, alpha fetoprotein (AFP), and c-reactive protein (CRP) were identified and included in an integrative risk prediction model. The AUC in overall population was 0.851 (95% CI = 0.840-0.862), with never smokers 0.806 (95% CI = 0.790-0.819), light smokers 0.847 (95% CI = 0.824-0.871), and heavy smokers 0.732 (95% CI = 0.708-0.752). By integrating risk factors such as family history of lung cancer, CEA and AFP for light smokers, and lung function test (Maximum Mid-Expiratory Flow, MMEF), AFP and CEA for never smokers, light and never smokers with cancer risks as high as those within heavy smokers could be identified. The risk model for heavy smokers can allow us to stratify heavy smokers into subgroups with distinct risks, which, if applied to low-dose computed tomography (LDCT) screening, may greatly reduce false positives.
本研究的目的是使用台湾的一个前瞻性队列 395875 名参与者,开发显著改善的肺癌风险预测模型。通过生成接收器工作曲线和估计曲线下面积(AUC)来衡量判别准确性。在多变量 Cox 回归分析中,年龄、性别、吸烟包年数、肺癌家族史、个人癌症史、BMI、肺功能测试以及癌胚抗原(CEA)、胆红素、甲胎蛋白(AFP)和 C-反应蛋白(CRP)等血清生物标志物被确定并纳入综合风险预测模型。总体人群的 AUC 为 0.851(95%CI=0.840-0.862),从不吸烟者为 0.806(95%CI=0.790-0.819),轻度吸烟者为 0.847(95%CI=0.824-0.871),重度吸烟者为 0.732(95%CI=0.708-0.752)。通过整合肺癌家族史、CEA 和 AFP 等风险因素用于轻度吸烟者,以及肺功能测试(最大中期呼气流量,MMEF)、AFP 和 CEA 用于从不吸烟者,可以识别出癌症风险与重度吸烟者相当的轻度和从不吸烟者。对于重度吸烟者的风险模型可以使我们将重度吸烟者细分为具有不同风险的亚组,如果应用于低剂量计算机断层扫描(LDCT)筛查,则可以大大减少假阳性。