França Giovanny V A, Restrepo-Méndez María Clara, Maia Maria Fátima S, Victora Cesar G, Barros Aluísio J D
International Center for Equity in Health, Federal University of Pelotas, Rua Marechal Deodoro, 1160 3° Piso, 96020-220, Pelotas, RS, Brazil.
Int J Equity Health. 2016 Nov 17;15(1):149. doi: 10.1186/s12939-016-0445-2.
The Brazilian SUS (Unified Health System) was created in 1988 within the new constitution, based on the premises of being universal, comprehensive, and equitable. The SUS offers free health care, independent of contribution or affiliation. Since then, great efforts and increasing investments have been made for the system to achieve its goals. We assessed how coverage and equity in selected reproductive and maternal interventions progressed in Brazil from 1986 to 2013.
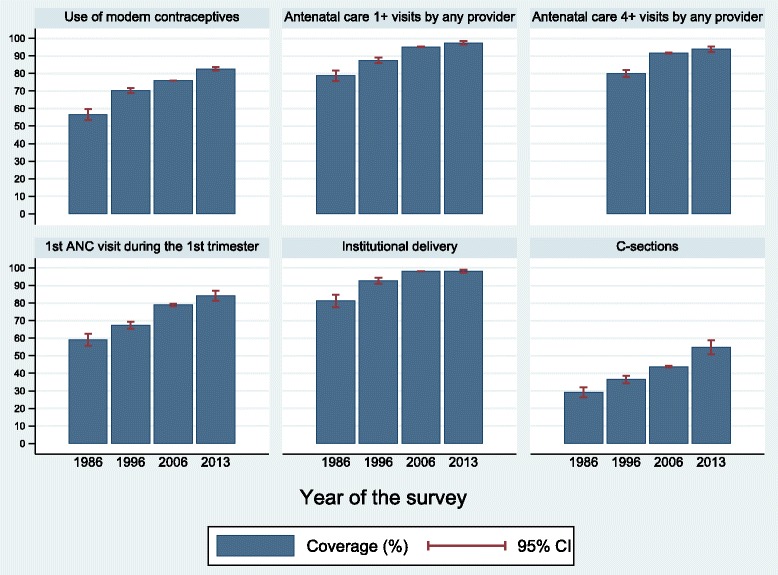
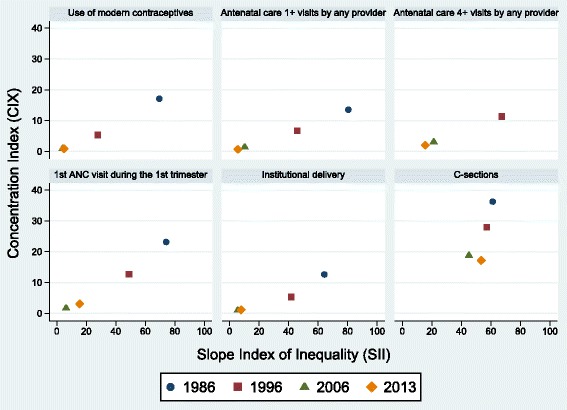
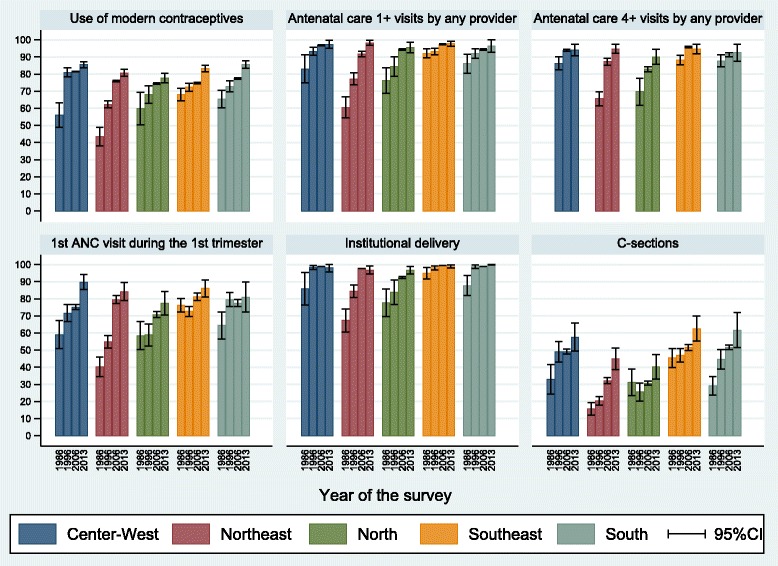
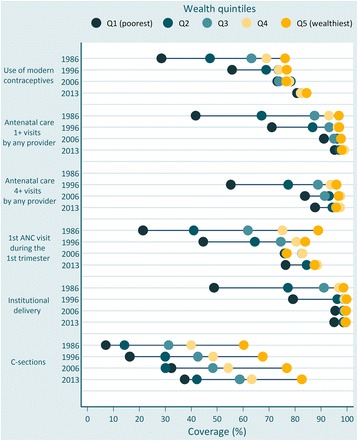
We reanalysed data from four national health surveys carried out in Brazil in 1986, 1996, 2006 and 2013. We estimated coverage for six interventions [use of modern contraceptives; antenatal care (ANC) 1+ visits by any provider; ANC 4+ visits by any provider; first ANC visit during the first trimester of pregnancy; institutional delivery; and Caesarean sections] using standard international definitions, and stratified results by wealth quintile, urban or rural residence and country regions. We also calculated two inequality indicators: the slope index of inequality (SII) and the concentration index (CIX).
All indicators showed steady increases in coverage over time. ANC 1+ and 4+ and institutional delivery reached coverage above 90 % in 2013. Prevalence of use of modern contraceptives was 83 % in 2013, indicating nearly universal satisfaction of need for contraception. On a less positive note, the proportion of C-sections has also grown continuously, reaching 55 % in 2013. There were marked reductions in wealth inequalities for all preventive interventions. Inequalities were significantly reduced for all indicators except for the C-section rate (p = 0.06), particularly in absolute terms (SII).
Despite the difficulties faced in the implementation of SUS, coverage of essential interventions increased and equity has improved dramatically, due in most cases to marked increase in coverage among the poorest 40 %. An increase in unnecessary Caesarean sections was also observed during the period. Further evaluation on the quality of healthcare provided is needed.
巴西统一卫生系统(SUS)于1988年依据新宪法设立,基于普遍性、全面性和公平性的原则。SUS提供免费医疗保健,与缴费或参保无关。自那时起,为使该系统实现其目标已付出巨大努力并不断增加投资。我们评估了1986年至2013年期间巴西在选定的生殖和孕产妇干预措施方面的覆盖情况及公平性进展。
我们重新分析了1986年、1996年、2006年和2013年在巴西开展的四次全国卫生调查的数据。我们使用标准国际定义估计了六种干预措施的覆盖情况[现代避孕方法的使用;任何提供者进行的1次及以上产前检查(ANC);任何提供者进行的4次及以上产前检查;孕期头三个月的首次产前检查;机构分娩;以及剖宫产],并按财富五分位数、城乡居住地和国家地区对结果进行分层。我们还计算了两个不平等指标:不平等斜率指数(SII)和集中指数(CIX)。
所有指标显示随着时间推移覆盖情况稳步上升。2013年,1次及以上和4次及以上产前检查以及机构分娩的覆盖率达到90%以上。2013年现代避孕方法的使用率为83%,表明避孕需求几乎得到普遍满足。不太乐观的是,剖宫产的比例也持续上升,2013年达到55%。所有预防性干预措施的财富不平等现象均显著减少。除剖宫产率外(p = 0.06),所有指标的不平等现象均显著减少,尤其是从绝对值(SII)来看。
尽管在实施SUS过程中面临困难,但基本干预措施的覆盖范围有所增加,公平性也有显著改善,在大多数情况下这归因于最贫困的40%人群的覆盖率显著提高。在此期间还观察到不必要剖宫产的增加。需要对所提供医疗保健的质量进行进一步评估。