Department of Data and Analytics, WHO, Geneve, Switzerland.
International Center for Equity in Health, Universidade Federal de Pelotas, Pelotas, Brazil.
BMJ Glob Health. 2020 Jan 26;5(1):e002229. doi: 10.1136/bmjgh-2019-002229. eCollection 2020.
Wealth-related inequalities in reproductive, maternal, neonatal and child health have been widely studied by dividing the population into quintiles. We present a comprehensive analysis of wealth inequalities for the composite coverage index (CCI) using national health surveys carried out since 2010, using wealth deciles and absolute income estimates as stratification variables, and show how these new approaches expand on traditional equity analyses.
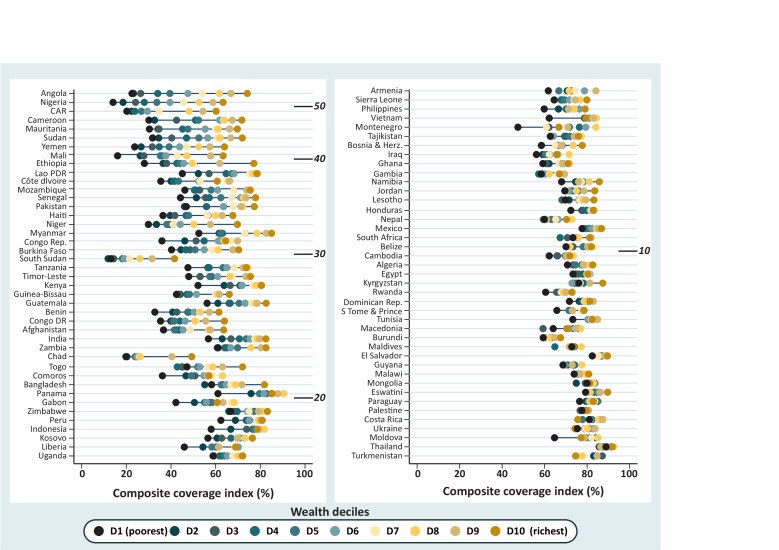
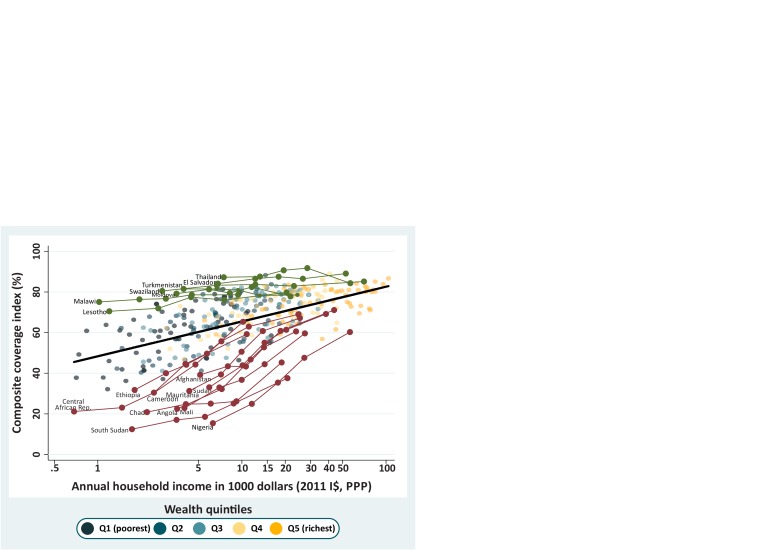
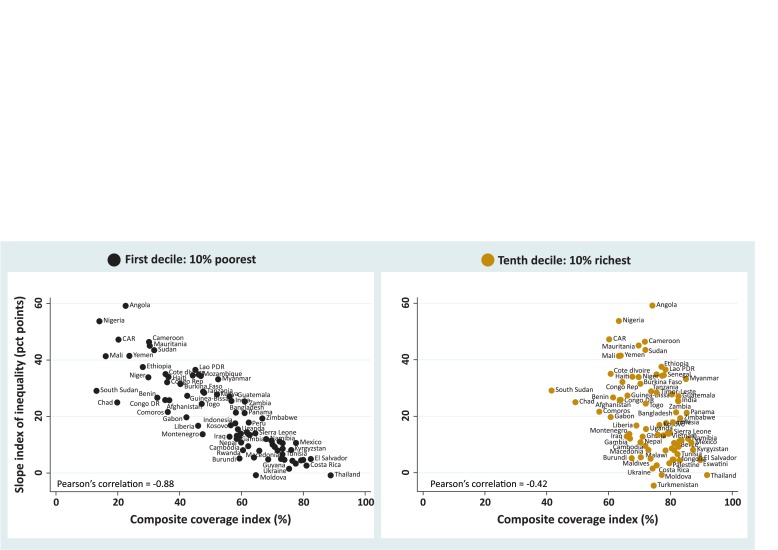
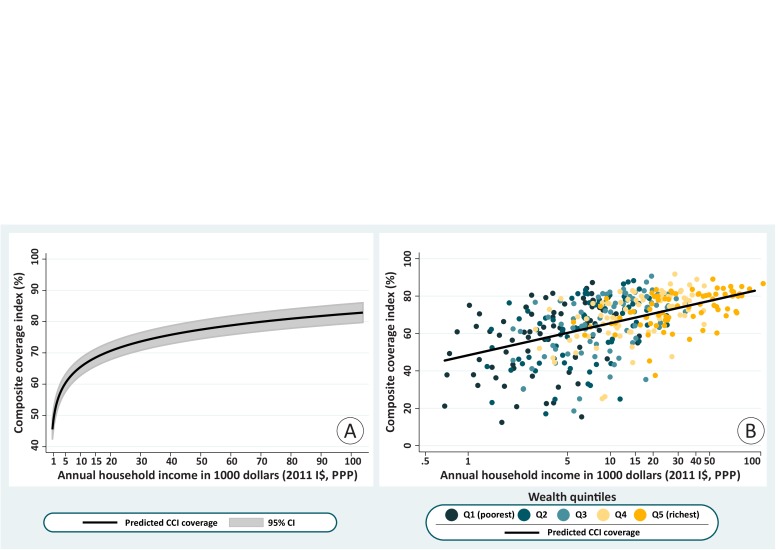
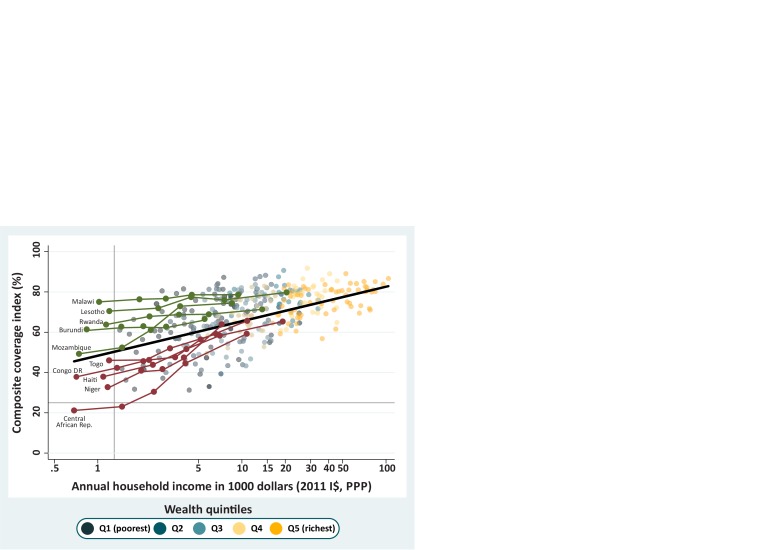
83 low-income and middle-income countries were studied. The CCI is a combined measure of coverage with eight key reproductive, maternal, newborn and child health interventions. It was disaggregated by wealth deciles for visual inspection of inequalities, and the slope index of inequality (SII) was estimated. The correlation between coverage in the extreme deciles and SII was assessed. Finally, we used multilevel models to examine how the CCI varies according to the estimated absolute income for each wealth quintile in the surveys.
The analyses of coverage by wealth deciles and by absolute income show that inequality is mostly driven by coverage among the poor, which is much more variable than coverage among the rich across countries. Regardless of national coverage, in 61 of the countries, the wealthiest decile achieved 70% or higher CCI coverage. Well-performing countries were particularly effective in achieving high coverage among the poor. In contrast, underperforming countries failed to reach the poorest, despite reaching the better-off.
There are huge inequalities between the richest and the poorest women and children in most countries. These inequalities are strongly driven by low coverage among the poorest given the wealthiest groups achieve high coverage irrespective of where they live, overcoming any barriers that are an impediment to others. Countries that 'punched above their weight' in coverage, given their level of absolute wealth, were those that best managed to reach their poorest women and children.
财富与生殖、孕产妇、新生儿和儿童健康之间的不平等关系已通过将人口分为五分位数进行了广泛研究。我们使用自 2010 年以来进行的国家健康调查,使用财富十分位数和绝对收入估计作为分层变量,对综合覆盖率指数(CCI)的财富不平等进行了全面分析,并展示了这些新方法如何扩展传统的公平分析。
研究了 83 个低收入和中等收入国家。CCI 是八项关键生殖、孕产妇、新生儿和儿童健康干预措施的综合覆盖率衡量标准。它按财富十分位数进行细分,以直观地观察不平等现象,并估计不平等斜率指数(SII)。评估了最极端十分位数的覆盖率与 SII 之间的相关性。最后,我们使用多水平模型来研究 CCI 如何根据调查中每个财富五分位数的估计绝对收入而变化。
对财富十分位数和绝对收入的覆盖率分析表明,不平等主要是由贫困人群的覆盖率驱动的,与各国的富裕人群相比,贫困人群的覆盖率变化更大。无论国家覆盖率如何,在 61 个国家中,最富有的十分位数的 CCI 覆盖率达到了 70%或更高。表现良好的国家在实现贫困人群的高覆盖率方面特别有效。相比之下,表现不佳的国家尽管覆盖了较富裕的人群,但未能覆盖到最贫困的人群。
在大多数国家,最富有的妇女和儿童与最贫穷的妇女和儿童之间存在巨大的不平等。鉴于最富有的群体无论居住在哪里都能获得高覆盖率,因此这些不平等主要是由最贫穷人群的低覆盖率驱动的,克服了对其他人构成障碍的任何障碍。在绝对财富水平下,在覆盖率方面“表现超出预期”的国家是那些最能设法覆盖其最贫困妇女和儿童的国家。