Wadman Renske I, Stam Marloes, Jansen Marc D, van der Weegen Yana, Wijngaarde Camiel A, Harschnitz Oliver, Sodaar Peter, Braun Kees P J, Dooijes Dennis, Lemmink Henny H, van den Berg Leonard H, van der Pol W Ludo
Brain Centre Rudolf Magnus, Department of Neurology and Neurosurgery, University Medical Centre Utrecht, Utrecht, The Netherlands.
Brain Centre Rudolf Magnus, Department of Neurology and Child Neurology, University Medical Centre Utrecht, Utrecht, The Netherlands.
PLoS One. 2016 Nov 28;11(11):e0167087. doi: 10.1371/journal.pone.0167087. eCollection 2016.
Clinical trials to test safety and efficacy of drugs for patients with spinal muscular atrophy (SMA) are currently underway. Biomarkers that document treatment-induced effects are needed because disease progression in childhood forms of SMA is slow and clinical outcome measures may lack sensitivity to detect meaningful changes in motor function in the period of 1-2 years of follow-up during randomized clinical trials.
To determine and compare SMN protein and mRNA levels in two cell types (i.e. PBMCs and skin-derived fibroblasts) from patients with SMA types 1-4 and healthy controls in relation to clinical characteristics and SMN2 copy numbers.
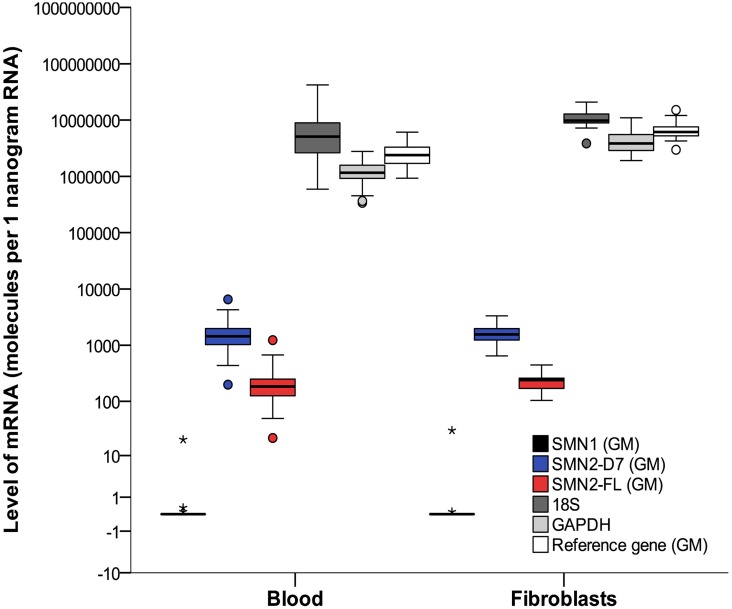
We determined SMN1, SMN2-full length (SMN2-FL), SMN2-delta7 (SMN2-Δ7), GAPDH and 18S mRNA levels and SMN protein levels in blood and fibroblasts from a total of 150 patients with SMA and 293 healthy controls using qPCR and ELISA. We analyzed the association with clinical characteristics including disease severity and duration, and SMN2 copy number.
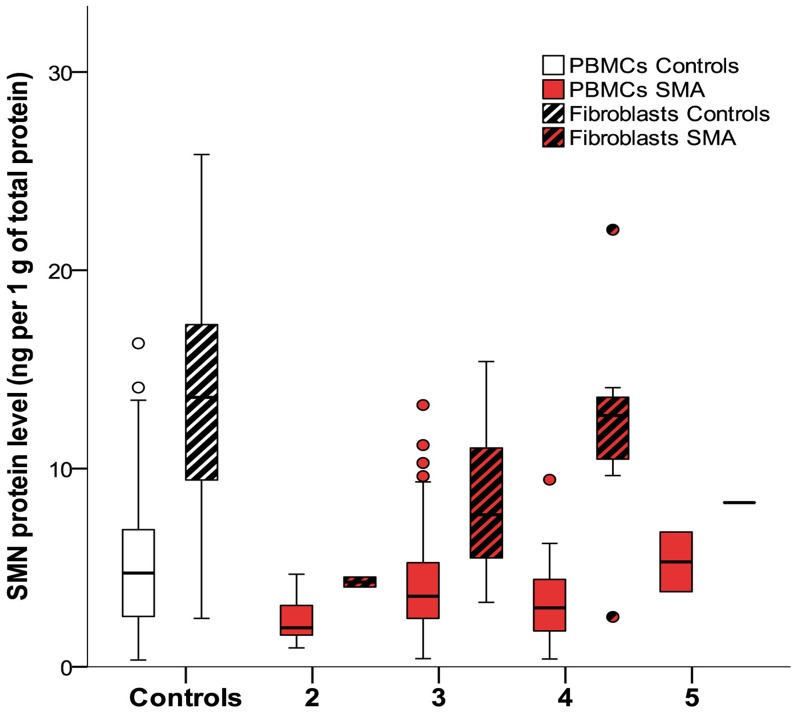
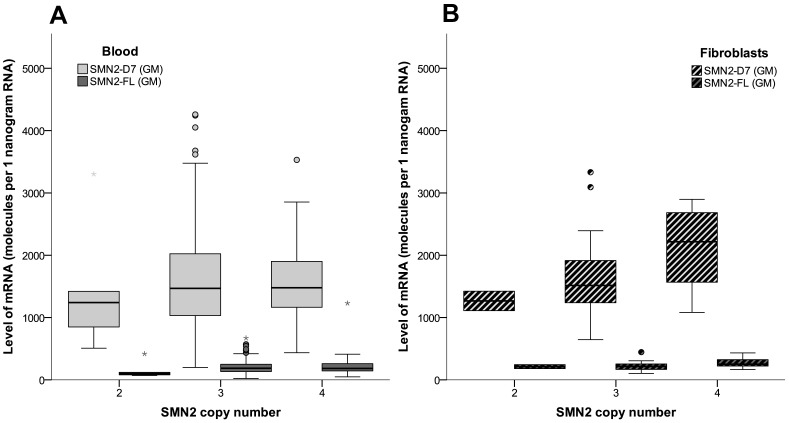
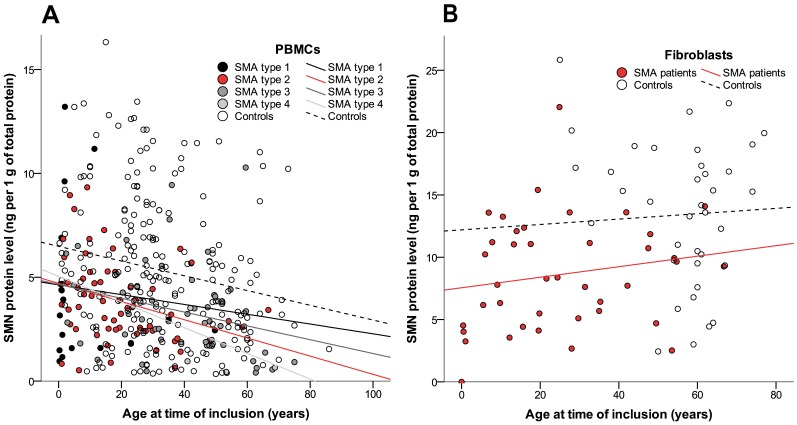
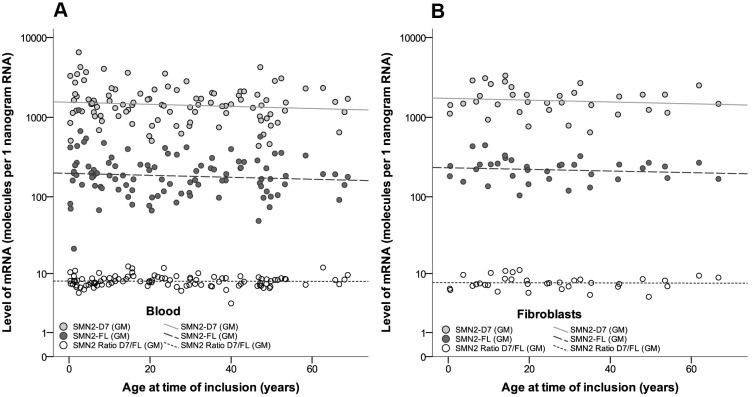
SMN protein levels in PBMCs and fibroblasts were higher in controls than in patients with SMA (p<0.01). Stratification for SMA type did not show differences in SMN protein (p>0.1) or mRNA levels (p>0.05) in either cell type. SMN2 copy number was associated with SMN protein levels in fibroblasts (p = 0.01), but not in PBMCs (p = 0.06). Protein levels in PBMCs declined with age in patients (p<0.01) and controls (p<0.01)(power 1-beta = 0.7). Ratios of SMN2-Δ7/SMN2-FL showed a broad range, primarily explained by the variation in SMN2-Δ7 levels, even in patients with a comparable SMN2 copy number. Levels of SMN2 mRNA did not correlate with SMN2 copy number, SMA type or age in blood (p = 0.7) or fibroblasts (p = 0.09). Paired analysis between blood and fibroblasts did not show a correlation between the two different tissues with respect to the SMN protein or mRNA levels.
SMN protein levels differ considerably between tissues and activity is age dependent in patients and controls. SMN protein levels in fibroblasts correlate with SMN2 copy number and have potential as a biomarker for disease severity.
目前正在进行测试治疗脊髓性肌萎缩症(SMA)患者药物安全性和有效性的临床试验。由于儿童型SMA的疾病进展缓慢,且在随机临床试验的1 - 2年随访期内,临床结局指标可能缺乏检测运动功能有意义变化的敏感性,因此需要能够记录治疗诱导效应的生物标志物。
确定并比较1 - 4型SMA患者和健康对照者两种细胞类型(即外周血单核细胞(PBMCs)和皮肤来源的成纤维细胞)中的SMN蛋白和mRNA水平,并分析其与临床特征及SMN2拷贝数的关系。
我们使用定量聚合酶链反应(qPCR)和酶联免疫吸附测定(ELISA),测定了总共150例SMA患者和293例健康对照者血液及成纤维细胞中的SMN1、全长SMN2(SMN2 - FL)、截短型SMN2(SMN2 - Δ7)、甘油醛 - 3 - 磷酸脱氢酶(GAPDH)和18S mRNA水平以及SMN蛋白水平。我们分析了其与包括疾病严重程度和病程等临床特征以及SMN2拷贝数的相关性。
PBMCs和成纤维细胞中的SMN蛋白水平在对照组中高于SMA患者(p < 0.01)。按SMA类型分层后,两种细胞类型中的SMN蛋白(p > 0.1)或mRNA水平(p > 0.05)均无差异。SMN2拷贝数与成纤维细胞中的SMN蛋白水平相关(p = 0.01),但与PBMCs中的无关(p = 0.06)。患者(p < 0.01)和对照组(p < 0.01)(检验效能1 - β = 0.7)的PBMCs中蛋白水平均随年龄下降。即使在SMN2拷贝数相当的患者中,SMN2 - Δ7/SMN2 - FL的比值范围也较宽,这主要由SMN2 - Δ7水平的变化所致。血液(p = 0.7)或成纤维细胞(p = 0.09)中SMN2 mRNA水平与SMN2拷贝数、SMA类型或年龄均无相关性。血液和成纤维细胞之间的配对分析未显示两种不同组织在SMN蛋白或mRNA水平上存在相关性。
组织间SMN蛋白水平差异显著,且在患者和对照中其活性均与年龄相关。成纤维细胞中的SMN蛋白水平与SMN2拷贝数相关,有潜力作为疾病严重程度的生物标志物。