Lund C M, Nielsen D, Dehlendorff C, Christiansen A B, Rønholt F, Johansen J S, Vistisen K K
Department of Medicine, Herlev and Gentofte Hospital, Copenhagen University, Herlev, Denmark; Department of Oncology, Herlev and Gentofte Hospital, Copenhagen University, Herlev, Denmark.
Department of Oncology, Herlev and Gentofte Hospital, Copenhagen University, Herlev, Denmark; Faculty of Health and Medical Sciences, Department of Clinical Medicine,Copenhagen University, Copenhagen, Denmark.
ESMO Open. 2016 Nov 14;1(5):e000087. doi: 10.1136/esmoopen-2016-000087. eCollection 2016.
Elderly patients with primary colorectal cancer (CRC) are less frequently treated with adjuvant chemotherapy than younger patients due to concerns regarding toxicity and efficiency. We investigated how age, performance status (PS) and comorbidity influence treatment outcomes.
A retrospective single-centre study of 529 patients with stages II-III CRC treated with adjuvant chemotherapy (5-fluorouracil/capecitabine+/÷oxaliplatin) from 2001 to 2011 at Herlev Hospital, Denmark. Baseline characteristics, chemotherapy and outcome were analysed with respect to age after adjusting for PS and comorbidity.
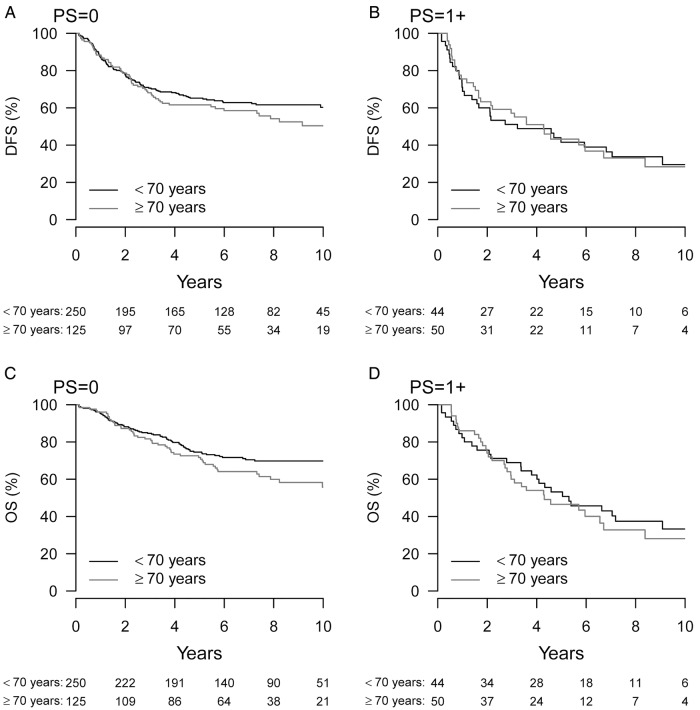
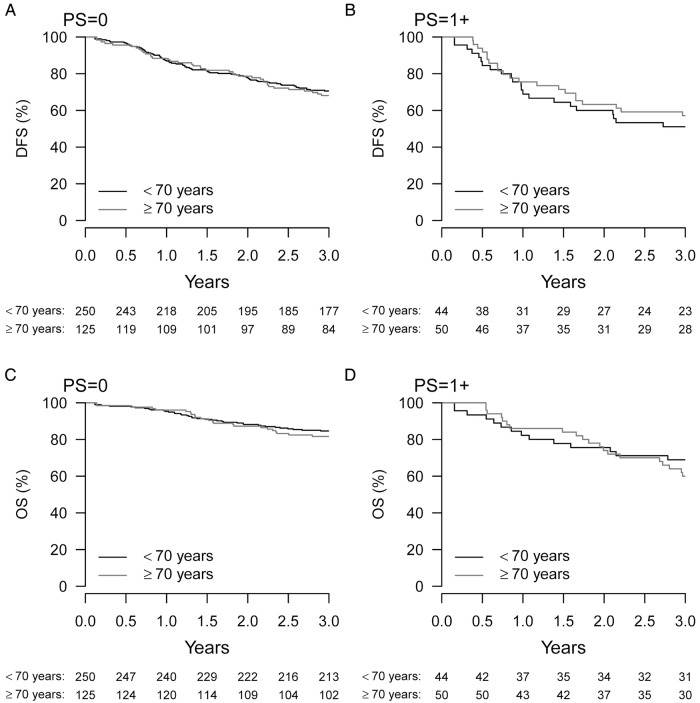
Elderly patients (>70 years) had significantly more comorbidity (p<0.001) and poorer PS (p=0.001) than younger patients. Elderly were more frequently treated with single-agent therapy (p=0.001) and at lower initial dose (p<0.001). There was no age-dependent difference in 3-year disease-free survival (DFS; HR 1.09, 95% CI 0.80 to 1.47, p=0.59), in grade 3-5 toxicity (29% vs 28%, p=0.86) or in 10-year CRC mortality (28%, HR 1.07, p=0.71). In elderly patients, a reduction in chemotherapy dose intensity compared with full dose had no impact on DFS or CRC mortality. Elderly patients receiving <50% of planned cycles had shorter DFS (HR=1.78, p=0.020) and higher CRC mortality (HR=2.17, p=0.027) than elderly receiving all cycles. Poor PS in younger and elderly patients was related to shorter DFS (HR=1.95, p=0.002; HR=1.6, p=0.035, respectively) and overall survival (OS; HR=2.28, p<0.001; HR=2.03, p=0.002). Comorbidity in younger patients was significantly related to shorter DFS (HR 2.72, p<0.001), OS (HR 3.16, p<0.001) and higher CRC mortality (HR 2.70, p=0.001).
Choice of regimen, primary dose reduction and given dose intensity in patients treated with adjuvant chemotherapy for CRC were highly dependent on age. However, age had no impact on DFS and CRC mortality. Comorbidity in younger patients and PS in all patients were associated with shorter DFS and higher CRC mortality.
由于对毒性和疗效的担忧,老年原发性结直肠癌(CRC)患者接受辅助化疗的频率低于年轻患者。我们研究了年龄、体能状态(PS)和合并症如何影响治疗结果。
对2001年至2011年在丹麦赫勒夫医院接受辅助化疗(5-氟尿嘧啶/卡培他滨+/-奥沙利铂)的529例II-III期CRC患者进行回顾性单中心研究。在调整PS和合并症后,分析年龄与基线特征、化疗及结果的关系。
老年患者(>70岁)的合并症显著多于年轻患者(p<0.001),PS也更差(p=0.001)。老年患者更常接受单药治疗(p=0.001)且初始剂量较低(p<0.001)。3年无病生存率(DFS;风险比1.09,95%置信区间0.80至1.47,p=0.59)、3-5级毒性(29%对28%,p=0.86)或10年CRC死亡率(28%,风险比1.07,p=0.71)均无年龄依赖性差异。在老年患者中,与全剂量相比化疗剂量强度降低对DFS或CRC死亡率无影响。接受计划周期<50%的老年患者的DFS短于接受所有周期的老年患者(风险比=1.78,p=0.020),CRC死亡率更高(风险比=2.17,p=0.027)。年轻和老年患者的PS差均与DFS缩短(风险比分别为1.95,p=0.002;1.6,p=0.035)和总生存期(OS;风险比分别为2.28,p<0.001;2.03,p=0.002)相关。年轻患者的合并症与DFS缩短(风险比2.72,p<0.001)、OS缩短(风险比3.16,p<0.001)及CRC死亡率升高(风险比2.70,p=0.001)显著相关。
CRC辅助化疗患者的方案选择、初始剂量降低及给药剂量强度高度依赖于年龄。然而,年龄对DFS和CRC死亡率无影响。年轻患者的合并症及所有患者的PS与DFS缩短和CRC死亡率升高相关。