Scialla Julia J, Asplin John, Dobre Mirela, Chang Alex R, Lash James, Hsu Chi-Yuan, Kallem Radhakrishna R, Hamm L Lee, Feldman Harold I, Chen Jing, Appel Lawrence J, Anderson Cheryl A M, Wolf Myles
Department of Medicine, Duke University School of Medicine, Durham, North Carolina, USA; Duke Clinical Research Institute, Duke University School of Medicine, Durham, North Carolina, USA; Department of Medicine, Durham Veterans Affairs Medical Center, Durham, North Carolina, USA.
Litholink Corp, Laboratory Corporation of America Holdings, Chicago, Illinois, USA.
Kidney Int. 2017 Jan;91(1):204-215. doi: 10.1016/j.kint.2016.09.012. Epub 2016 Dec 1.
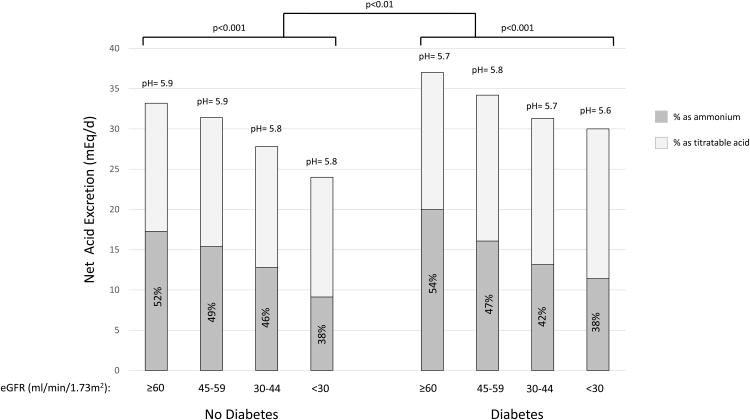
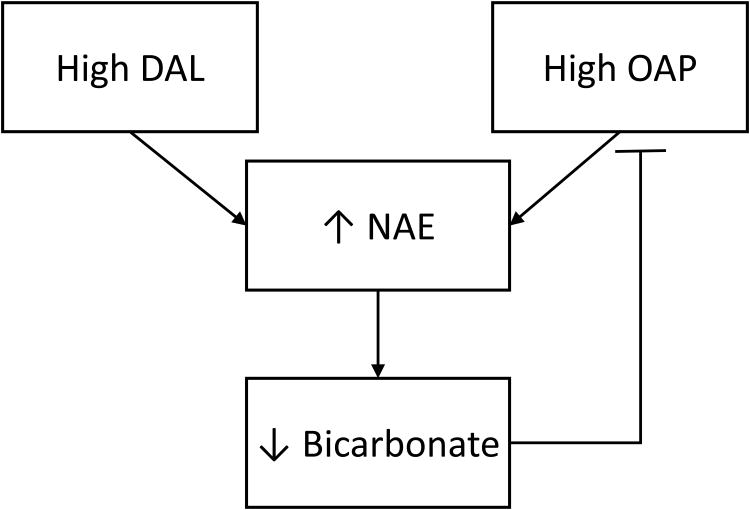
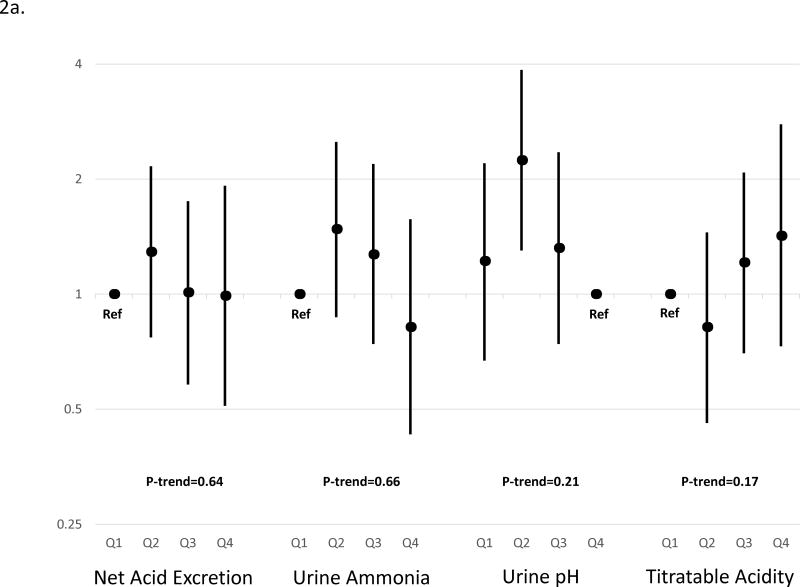
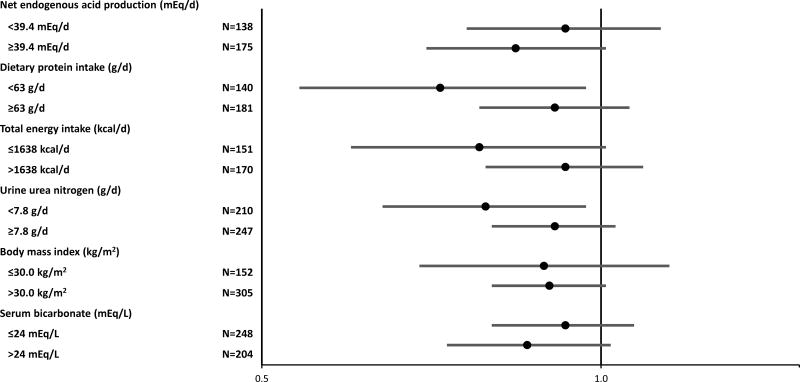
Higher diet-dependent nonvolatile acid load is associated with faster chronic kidney disease (CKD) progression, but most studies have used estimated acid load or measured only components of the gold standard, net acid excretion (NAE). Here we measured NAE as the sum of urine ammonium and titratable acidity in 24-hour urines from a random subset of 980 participants in the Chronic Renal Insufficiency Cohort (CRIC) Study. In multivariable models accounting for demographics, comorbidity and kidney function, higher NAE was significantly associated with lower serum bicarbonate (0.17 mEq/l lower serum bicarbonate per 10 mEq/day higher NAE), consistent with a larger acid load. Over a median of 6 years of follow-up, higher NAE was independently associated with a significantly lower risk of the composite of end-stage renal disease or halving of estimated glomerular filtration rate among diabetics (hazard ratio 0.88 per 10 mEq/day higher NAE), but not those without diabetes (hazard ratio 1.04 per 10 mEq/day higher NAE). For comparison, we estimated the nonvolatile acid load as net endogenous acid production using self-reported food frequency questionnaires from 2848 patients and dietary urine biomarkers from 3385 patients. Higher net endogenous acid production based on biomarkers (urea nitrogen and potassium) was modestly associated with faster CKD progression consistent with prior reports, but only among those without diabetes. Results from the food frequency questionnaires were not associated with CKD progression in any group. Thus, disparate results obtained from analyses of nonvolatile acid load directly measured as NAE and estimated from diet suggest a novel hypothesis that the risk of CKD progression related to low NAE or acid load may be due to diet-independent changes in acid production in diabetes.
更高的饮食依赖性非挥发性酸负荷与慢性肾脏病(CKD)进展更快相关,但大多数研究使用的是估计酸负荷或仅测量了金标准净酸排泄(NAE)的组成部分。在此,我们在慢性肾功能不全队列(CRIC)研究的980名参与者的随机子集中,测量了24小时尿液中NAE(尿液铵和可滴定酸度之和)。在考虑人口统计学、合并症和肾功能的多变量模型中,较高的NAE与较低的血清碳酸氢盐显著相关(NAE每升高10 mEq/天,血清碳酸氢盐降低0.17 mEq/l),这与更大的酸负荷一致。在中位6年的随访中,较高的NAE与糖尿病患者终末期肾病或估计肾小球滤过率减半的复合终点风险显著降低独立相关(NAE每升高10 mEq/天,风险比为0.88),但在非糖尿病患者中并非如此(NAE每升高10 mEq/天,风险比为1.04)。为作比较,我们使用2848例患者的自我报告食物频率问卷和3385例患者的饮食尿液生物标志物,将非挥发性酸负荷估计为净内源性酸产生。基于生物标志物(尿素氮和钾)的较高净内源性酸产生与CKD进展更快适度相关,这与先前报告一致,但仅在非糖尿病患者中如此。食物频率问卷的结果在任何组中均与CKD进展无关。因此,通过直接测量为NAE的非挥发性酸负荷分析和从饮食估计得到的不同结果提示了一个新的假说,即与低NAE或酸负荷相关的CKD进展风险可能归因于糖尿病患者酸产生的饮食非依赖性变化。