Tyagi Neelam, Sutton Elizabeth, Hunt Margie, Zhang Jing, Oh Jung Hun, Apte Aditya, Mechalakos James, Wilgucki Molly, Gelb Emily, Mehrara Babak, Matros Evan, Ho Alice
Department of Medical Physics, Memorial Sloan Kettering Cancer Center, New York, New York.
Department of Radiology, Memorial Sloan Kettering Cancer Center, New York, New York.
Int J Radiat Oncol Biol Phys. 2017 Feb 1;97(2):411-419. doi: 10.1016/j.ijrobp.2016.09.041. Epub 2016 Oct 6.
Capsular contracture (CC) is a serious complication in patients receiving implant-based reconstruction for breast cancer. Currently, no objective methods are available for assessing CC. The goal of the present study was to identify image-based surrogates of CC using magnetic resonance imaging (MRI).
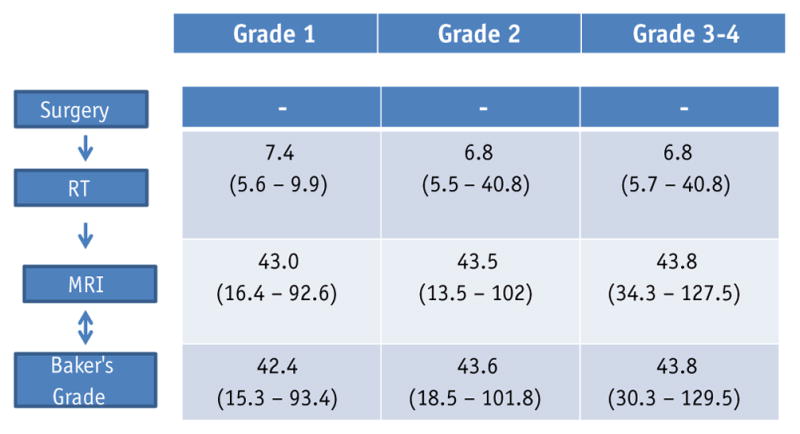
We analyzed a retrospective data set of 50 patients who had undergone both a diagnostic MRI scan and a plastic surgeon's evaluation of the CC score (Baker's score) within a 6-month period after mastectomy and reconstructive surgery. The MRI scans were assessed for morphologic shape features of the implant and histogram features of the pectoralis muscle. The shape features, such as roundness, eccentricity, solidity, extent, and ratio length for the implant, were compared with the Baker score. For the pectoralis muscle, the muscle width and median, skewness, and kurtosis of the intensity were compared with the Baker score. Univariate analysis (UVA) using a Wilcoxon rank-sum test and multivariate analysis with the least absolute shrinkage and selection operator logistic regression was performed to determine significant differences in these features between the patient groups categorized according to their Baker's scores.
UVA showed statistically significant differences between grade 1 and grade ≥2 for morphologic shape features and histogram features, except for volume and skewness. Only eccentricity, ratio length, and volume were borderline significant in differentiating grade ≤2 and grade ≥3. Features with P<.1 on UVA were used in the multivariate least absolute shrinkage and selection operator logistic regression analysis. Multivariate analysis showed a good level of predictive power for grade 1 versus grade ≥2 CC (area under the receiver operating characteristic curve 0.78, sensitivity 0.78, and specificity 0.82) and for grade ≤2 versus grade ≥3 CC (area under the receiver operating characteristic curve 0.75, sensitivity 0.75, and specificity 0.79).
The morphologic shape features described on MR images were associated with the severity of CC. MRI has the potential to further improve the diagnostic ability of the Baker score in breast cancer patients who undergo implant reconstruction.
包膜挛缩(CC)是接受乳腺癌植入物重建患者的一种严重并发症。目前,尚无客观方法可用于评估CC。本研究的目的是使用磁共振成像(MRI)确定基于图像的CC替代指标。
我们分析了50例患者的回顾性数据集,这些患者在乳房切除和重建手术后6个月内接受了诊断性MRI扫描以及整形外科医生对CC评分(贝克评分)的评估。对MRI扫描评估植入物的形态形状特征和胸大肌的直方图特征。将植入物的形状特征,如圆度、偏心率、紧实度、范围和长宽比,与贝克评分进行比较。对于胸大肌,将肌肉宽度以及强度的中位数、偏度和峰度与贝克评分进行比较。使用Wilcoxon秩和检验进行单变量分析(UVA),并使用最小绝对收缩和选择算子逻辑回归进行多变量分析,以确定根据贝克评分分类的患者组之间这些特征的显著差异。
UVA显示,除体积和偏度外,形态形状特征和直方图特征在1级和≥2级之间存在统计学显著差异。在区分≤2级和≥3级时,只有偏心率、长宽比和体积具有临界显著性。UVA中P<0.1的特征用于多变量最小绝对收缩和选择算子逻辑回归分析。多变量分析显示,对于1级与≥2级CC(受试者操作特征曲线下面积为0.78,灵敏度为0.78,特异性为0.82)以及≤2级与≥3级CC(受试者操作特征曲线下面积为0.75,灵敏度为0.75,特异性为0.79)具有良好的预测能力。
MR图像上描述的形态形状特征与CC的严重程度相关。MRI有可能进一步提高接受植入物重建的乳腺癌患者中贝克评分的诊断能力。