Kinoshita Maho, Morioka Nobutada, Yabuuchi Mariko, Ozaki Makoto
Department of Anesthesiology, Tokyo Women's Medical University, Shinjuku, Tokyo, 1628666, Japan.
J Anesth. 2017 Apr;31(2):198-205. doi: 10.1007/s00540-016-2290-2. Epub 2016 Dec 19.
There is still no easy and highly useful method to comprehensively assess both preoperative and intraoperative patient statuses to predict postoperative outcomes. We attempted to develop a new scoring system that would enable a comprehensive assessment of preoperative and intraoperative patient statuses instantly at the end of anesthesia, predicting postoperative mortality.
The study included 32,555 patients who underwent surgery under general or regional anesthesia from 2008 to 2012. From the anesthesia records, extracted factors, including patient characteristics and American Society of Anesthesiologists physical status classification (ASA-PS), and three intraoperative indexes (the lowest heart rate, lowest mean arterial pressure, and estimated volume of blood loss) are used to calculate the surgical Apgar score (sAs). The sAs and ASA-PS, and surgical Apgar score combined with American Society of Anesthesiologists physical status classification (SASA), which combines the sAs and ASA-PS into a single adjusted scale, were compared and analyzed with postoperative 30-day mortality.
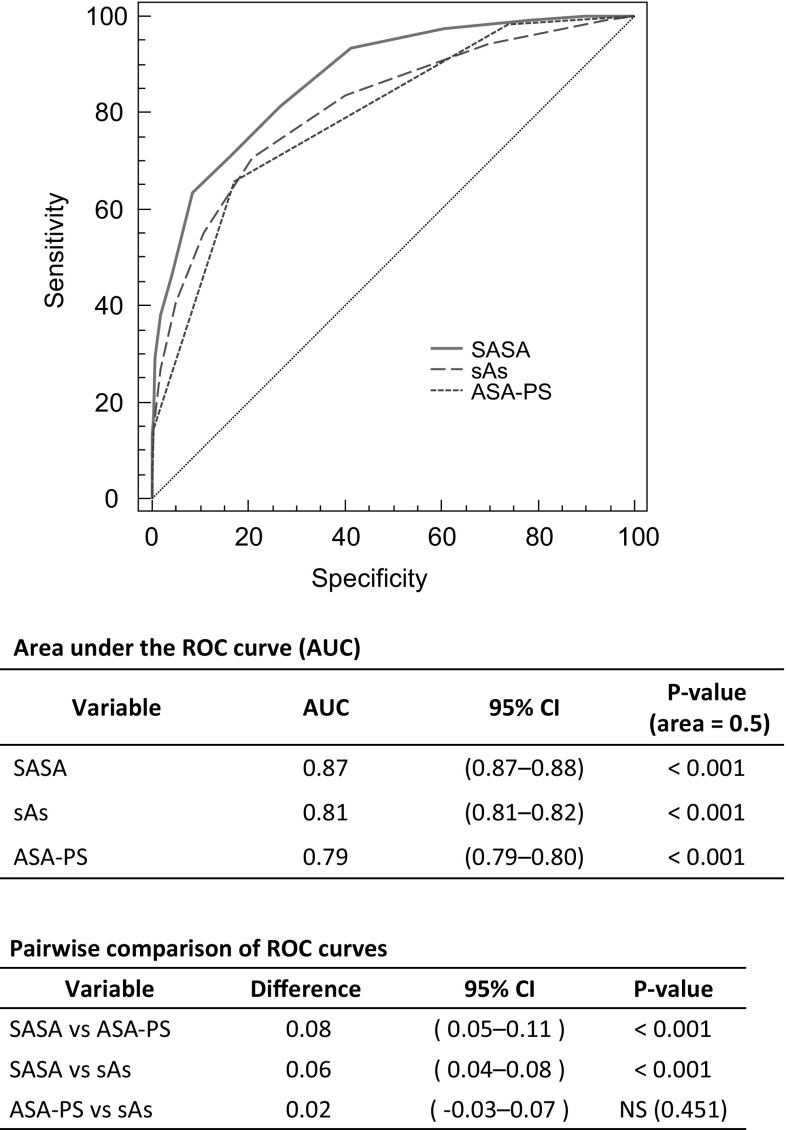
Increased severity of the sAs, ASA-PS and SASA was correlated with significantly higher mortality. The risk of death was elevated by 3.65 for every 2-point decrease in the sAs, by 6.4 for every 1-point increase in the ASA-PS, and by 9.56 for every 4-point decrease in the SASA. The ROC curves of the sAs and ASA-PS alone also individually demonstrated high validity (AUC = 0.81 for sAs and 0.79 for ASA-PS, P < 0.001). The SASA was even more valid (AUC = 0.87, P < 0.001).
The sAs and ASA-PS were shown to be extremely useful for predicting 30-day mortality after surgery. An even higher predictive ability was demonstrated by the SASA, which combines these simple and effective scoring systems.
目前仍没有一种简单且非常有用的方法能够全面评估术前和术中患者的状态以预测术后结果。我们试图开发一种新的评分系统,该系统能够在麻醉结束时即刻全面评估术前和术中患者的状态,预测术后死亡率。
本研究纳入了2008年至2012年期间接受全身麻醉或区域麻醉手术的32555例患者。从麻醉记录中提取包括患者特征和美国麻醉医师协会身体状况分类(ASA-PS)在内的因素,以及三个术中指标(最低心率、最低平均动脉压和估计失血量),用于计算手术Apgar评分(sAs)。将sAs和ASA-PS,以及将sAs和ASA-PS合并为单一调整量表的手术Apgar评分与美国麻醉医师协会身体状况分类相结合(SASA),与术后30天死亡率进行比较和分析。
sAs、ASA-PS和SASA严重程度的增加与显著更高的死亡率相关。sAs每降低2分,死亡风险升高3.65;ASA-PS每升高1分,死亡风险升高6.4;SASA每降低4分,死亡风险升高9.56。单独的sAs和ASA-PS的ROC曲线也分别显示出高有效性(sAs的AUC = 0.81,ASA-PS的AUC = 0.79,P < 0.001)。SASA的有效性更高(AUC = 0.87,P < 0.001)。
sAs和ASA-PS被证明对预测术后30天死亡率非常有用。将这些简单有效的评分系统结合起来的SASA显示出更高的预测能力。