Hariyanto Hori, Yahya Corry Quando, Wibowo Primartanto, Tampubolon Oloan E
Department of Anesthesiology and Critical Care Medicine, 3rd floor, Siloam Hospitals Lippo Village, Jalan Siloam No. 6, Karawaci, 15811, Tangerang, Banten, Indonesia.
Department of Anesthesiology, Universitas Pelita Harapan Faculty of Medicine, Jalan Boulevard Jendral Sudirman, Lippo Karawaci, Tangerang, 15811, Indonesia.
J Med Case Rep. 2016 Dec 20;10(1):357. doi: 10.1186/s13256-016-1129-7.
The incidence of dengue hemorrhagic fever is increasing among the adult population living in endemic areas. The disease carries a 0.73% fatality rate for the general population, but what happens when the disease strikes a special subpopulation group, the obstetrics? Perhaps the important question specific to this special subpopulation revolves around the right time and mode of delivery under severe coagulopathy and plasma leakage in conditions of imminent delivery.
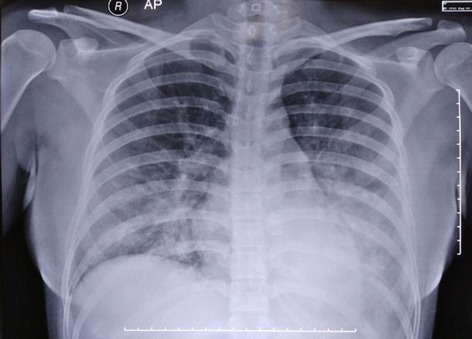
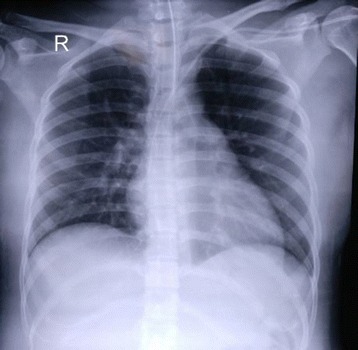
A 24-year-old primigravid Sundanese woman presented to our intensive care unit due to acute pulmonary edema secondary to massive plasma leakage caused by severe dengue. She tested positive for both immunoglobulin G and immunoglobulin M dengue serology indicating she had secondary dengue infection, which placed her at risk for an exaggerated cytokine response as was evident clinically. She had to undergo an emergency cesarean section which was later complicated by rebleeding and hemodynamic instability due to an atypical defervescence period. She was successfully managed by multiple blood transfusions and was discharged from our intensive care unit on day 8 without any negative sequel.
Fever, thrombocytopenia, and hemoconcentration are the classical symptoms of dengue hemorrhagic fever observed in adult, pediatric, and obstetric populations. However, a clinician must be particularly watchful in treating a pregnant dengue-infected patient as physiologic hematology changes provide greater volume compensation and the advent of shock marks significant volume loss. In conclusion, an important principle in the management of dengue hemorrhagic fever in pregnancy is to prioritize maternal well-being prior to addressing fetal issues.
在流行地区的成年人群中,登革出血热的发病率正在上升。该疾病在普通人群中的病死率为0.73%,但当这种疾病侵袭一个特殊的亚人群——产科患者时会发生什么呢?也许针对这个特殊亚人群的重要问题围绕着在即将分娩的情况下,严重凝血障碍和血浆渗漏时的正确分娩时间和方式。
一名24岁的巽他族初产妇因严重登革热导致大量血浆渗漏继发急性肺水肿,被送至我们的重症监护病房。她的登革热血清学检测免疫球蛋白G和免疫球蛋白M均呈阳性,表明她有二次登革热感染,临床上明显可见这使她有发生过度细胞因子反应的风险。她不得不接受紧急剖宫产,随后因非典型退热期出现再出血和血流动力学不稳定。通过多次输血她得到了成功救治,并于第8天从我们的重症监护病房出院,没有任何不良后遗症。
发热、血小板减少和血液浓缩是在成人、儿童和产科人群中观察到的登革出血热的典型症状。然而,临床医生在治疗感染登革热的孕妇时必须格外警惕,因为生理血液学变化提供了更大的容量代偿,而休克的出现标志着大量的容量丧失。总之,妊娠期登革出血热管理的一个重要原则是在处理胎儿问题之前优先考虑母亲的健康。