Russell Christopher J, Mack Wendy J, Schrager Sheree M, Wu Susan
Department of Pediatrics and
Division of Hospital Medicine, Children's Hospital Los Angeles, Los Angeles, California.
Hosp Pediatr. 2017 Jan;7(1):16-23. doi: 10.1542/hpeds.2016-0104.
Identify hospital-level care variations and association with length of stay (LOS) and hospital revisit in children with tracheostomies hospitalized for bacterial respiratory tract infections (bRTIs).
A multicenter, retrospective cohort study that used the Pediatric Health Information System database between 2007 and 2014 of patients with tracheostomies aged ≤18 years with a primary diagnosis of bRTI (eg, tracheitis) or a primary diagnosis of a bRTI symptom (eg, cough) and a secondary diagnosis of bRTI. Primary outcomes were LOS and 30-day all-cause revisit rates. Secondary outcomes included hospital-level diagnostic testing and anti-Pseudomonas antibiotic use. We used mixed-effects negative binomial (for LOS) and logistic (for revisit) regression to explore the relationship between hospital-level diagnostic test utilization and the outcomes.
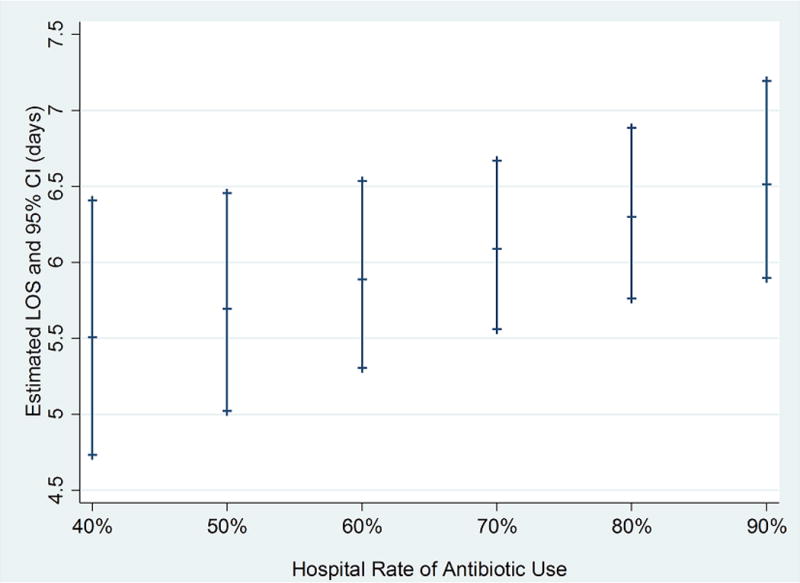
Data representing 4137 unique patients with a median age of 3 years (interquartile range: 1-9 years) were included. Median LOS was 4 days (interquartile range: 3-8 days), and the 30-day revisit rate was 24.9%. Use of diagnostic testing and empirical anti-Pseudomonas antibiotics varied significantly among hospitals (all P values <.001). After adjusting for patient and hospital characteristics, compared with low test utilization hospitals, there were no differences in 30-day all-cause revisit rates in moderate (adjusted odds ratio: 1.19; 95% confidence interval [CI]: 0.93-1.52) or high (adjusted odds ratio: 1.07; 95% CI: 0.82-1.39) utilization hospitals. LOS in hospitals with moderate (% difference: -0.8%; 95% CI: -14.4-14.9%) or high (% difference: 13.9%; 95% CI: -0.7-30.6%) test utilization was not significantly longer.
Given that care variations were not associated with outcomes, future research should focus on standardizing diagnosis and treatment of bRTIs and readmission prevention in this population.
确定因细菌性呼吸道感染(bRTIs)住院的气管切开患儿在医院层面的护理差异以及与住院时间(LOS)和再次入院的关联。
一项多中心回顾性队列研究,使用2007年至2014年期间儿科健康信息系统数据库中年龄≤18岁、主要诊断为bRTI(如气管炎)或主要诊断为bRTI症状(如咳嗽)且次要诊断为bRTI的气管切开患者。主要结局为住院时间和30天全因再次入院率。次要结局包括医院层面的诊断性检查和抗假单胞菌抗生素使用情况。我们使用混合效应负二项式回归(用于住院时间)和逻辑回归(用于再次入院)来探讨医院层面诊断性检查利用与结局之间的关系。
纳入了代表4137例独特患者的数据,中位年龄为3岁(四分位间距:1 - 9岁)。中位住院时间为4天(四分位间距:3 - 8天),30天再次入院率为24.9%。医院之间诊断性检查和经验性抗假单胞菌抗生素的使用差异显著(所有P值<.001)。在调整患者和医院特征后,与低检查利用率医院相比,中度(调整后的优势比:1.19;95%置信区间[CI]:0.93 - 1.52)或高度(调整后的优势比:1.07;95% CI:0.82 - 1.39)利用率医院的30天全因再次入院率没有差异。中度(差异百分比:-0.8%;95% CI:-14.4 - 14.9%)或高度(差异百分比:13.9%;95% CI:-0.7 - 30.6%)检查利用率医院的住院时间没有显著延长。
鉴于护理差异与结局无关,未来研究应专注于该人群中bRTIs的诊断和治疗标准化以及再入院预防。