Kong Lin, Gao Jing, Hu Jiyi, Hu Weixu, Guan Xiyin, Lu Rong, Lu Jiade J
Department of Radiation Oncology, Shanghai Proton and Heavy Ion Center, Fudan University Shanghai Cancer Hospital, Shanghai, 200321, P. R. China.
Department of Radiation Oncology, Shanghai Proton and Heavy Ion Center, Shanghai, 200321, P. R. China.
Chin J Cancer. 2016 Dec 22;35(1):101. doi: 10.1186/s40880-016-0164-5.
After definitive chemoradiotherapy for non-metastatic nasopharyngeal carcinoma (NPC), more than 10% of patients will experience a local recurrence. Salvage treatments present significant challenges for locally recurrent NPC. Surgery, stereotactic ablative body radiotherapy, and brachytherapy have been used to treat locally recurrent NPC. However, only patients with small-volume tumors can benefit from these treatments. Re-irradiation with X-ray-based intensity-modulated radiotherapy (IMXT) has been more widely used for salvage treatment of locally recurrent NPC with a large tumor burden, but over-irradiation to the surrounding normal tissues has been shown to cause frequent and severe toxicities. Furthermore, locally recurrent NPC represents a clinical entity that is more radio-resistant than its primary counterpart. Due to the inherent physical advantages of heavy-particle therapy, precise dose delivery to the target volume(s), without exposing the surrounding organs at risk to extra doses, is highly feasible with carbon-ion radiotherapy (CIRT). In addition, CIRT is a high linear energy transfer (LET) radiation and provides an increased relative biological effectiveness compared with photon and proton radiotherapy. Our prior work showed that CIRT alone to 57.5 GyE (gray equivalent), at 2.5 GyE per daily fraction, was well tolerated in patients who were previously treated for NPC with a definitive dose of IMXT. The short-term response rates at 3-6 months were also acceptable. However, no patients were treated with concurrent chemotherapy. Whether the addition of concurrent chemotherapy to CIRT can benefit locally recurrent NPC patients over CIRT alone has never been addressed. It is possible that the benefits of high-LET CIRT may make radiosensitizing chemotherapy unnecessary. We therefore implemented a phase I/II clinical trial to address these questions and present our methodology and results.
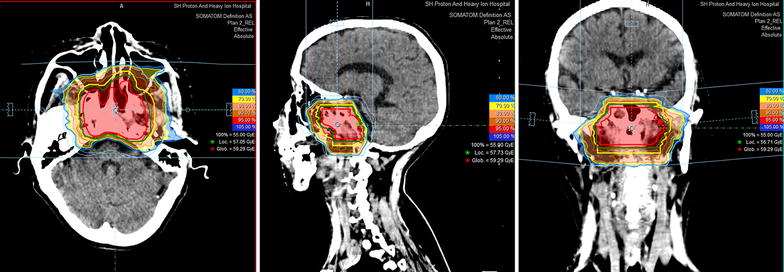
The maximal tolerated dose (MTD) of re-treatment using raster-scanning CIRT plus concurrent cisplatin will be determined in the phase I, dose-escalating stage of this study. CIRT dose escalation from 52.5 to 65 GyE (2.5 GyE × 21-26 fractions) will be delivered, with the primary endpoints being acute and subacute toxicities. Efficacy in terms of overall survival (OS) and local progression-free survival of patients after concurrent chemotherapy plus CIRT at the determined MTD will then be studied in the phase II stage of the trial. We hypothesize that CIRT plus chemotherapy can improve the 2-year OS rate from the historical 50% to at least 70%.
Re-treatment of locally recurrent NPC using photon radiation techniques, including IMXT, provides moderate efficacy but causes potentially severe toxicities. Improved outcomes in terms of efficacy and toxicity profile are expected with CIRT plus chemotherapy. However, the MTD of CIRT used concurrently with cisplatin-based chemotherapy for locally recurrent NPC remains to be determined. In addition, whether the addition of chemotherapy to CIRT is needed remains unknown. These questions will be evaluated in the dose-escalating phase I and randomized phase II trials.
在对非转移性鼻咽癌(NPC)进行确定性放化疗后,超过10%的患者会出现局部复发。挽救性治疗对局部复发的NPC构成重大挑战。手术、立体定向消融体部放疗和近距离放疗已被用于治疗局部复发的NPC。然而,只有小体积肿瘤患者能从这些治疗中获益。基于X射线的调强放疗(IMXT)再程放疗已更广泛地用于挽救治疗肿瘤负荷大的局部复发NPC,但对周围正常组织的过度照射已被证明会导致频繁且严重的毒性反应。此外,局部复发的NPC是一种比其原发灶更具放射抗性的临床实体。由于重粒子治疗固有的物理优势,碳离子放疗(CIRT)能够高度精确地将剂量传递至靶区,而不会使周围危及器官受到额外剂量照射。此外,CIRT是一种高传能线密度(LET)辐射,与光子和质子放疗相比,其相对生物效应增加。我们之前的研究表明,对于先前接受过确定性剂量IMXT治疗的NPC患者,单独给予CIRT至57.5 GyE(戈瑞当量),每日分次剂量为2.5 GyE,耐受性良好。3至6个月时的短期缓解率也可接受。然而,没有患者接受同步化疗。CIRT联合同步化疗是否比单纯CIRT更能使局部复发的NPC患者获益,这一问题从未得到解决。有可能高LET的CIRT的益处使得放射增敏化疗变得不必要。因此,我们开展了一项I/II期临床试验来解决这些问题,并展示我们的方法和结果。
在本研究的I期剂量递增阶段,将确定使用光栅扫描CIRT联合顺铂进行再治疗的最大耐受剂量(MTD)。CIRT剂量将从52.5 GyE递增至65 GyE(2.5 GyE×21 - 26次分割),主要终点为急性和亚急性毒性反应。然后在试验的II期阶段研究在确定的MTD下同步化疗加CIRT后患者的总生存期(OS)和局部无进展生存期方面的疗效。我们假设CIRT加化疗可将2年OS率从历史上的50%提高至至少70%。
使用包括IMXT在内的光子放疗技术对局部复发的NPC进行再治疗,疗效中等,但会导致潜在的严重毒性反应。预计CIRT加化疗在疗效和毒性方面会有更好的结果。然而,CIRT与基于顺铂的化疗联合用于局部复发NPC的MTD仍有待确定。此外,CIRT是否需要联合化疗尚不清楚。这些问题将在剂量递增的I期和随机II期试验中进行评估。