Sheikh Aadam, Dhami Sangeeta, Regent Lynne, Austin Moira, Sheikh Aziz
University College London, London WC1E 6BT, UK.
Edinburgh EH17 8UD, UK.
JRSM Open. 2015 Jul 28;6(7):2054270415593443. doi: 10.1177/2054270415593443. eCollection 2015 Jul.
To examine the circumstances, features and management of anaphylaxis in children and adults.
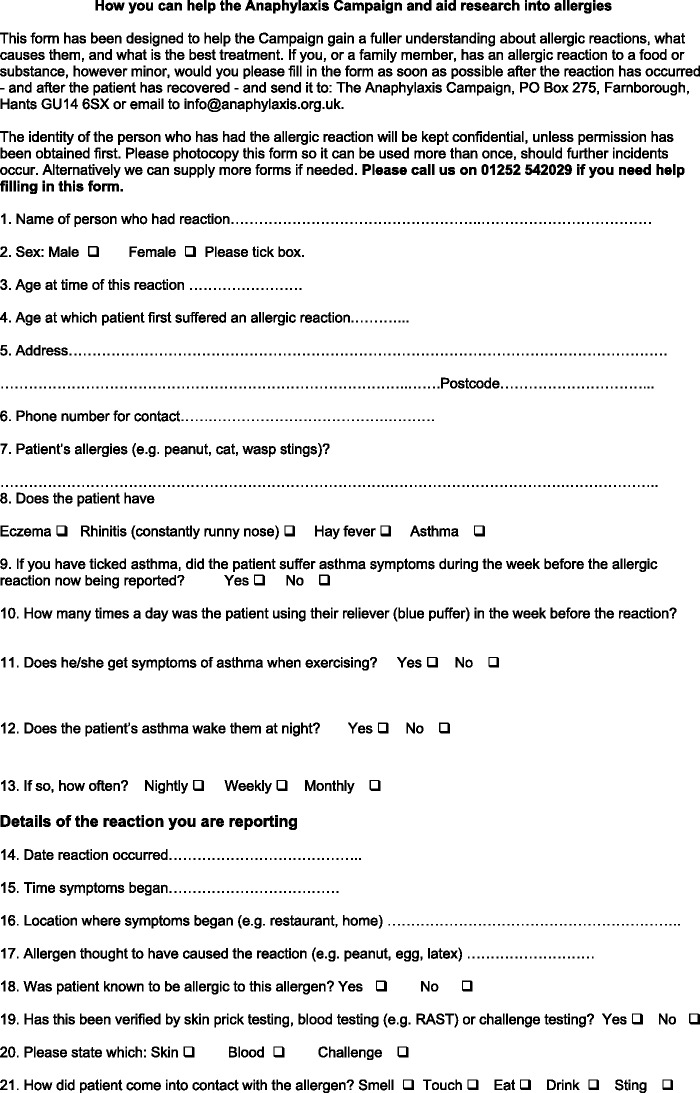
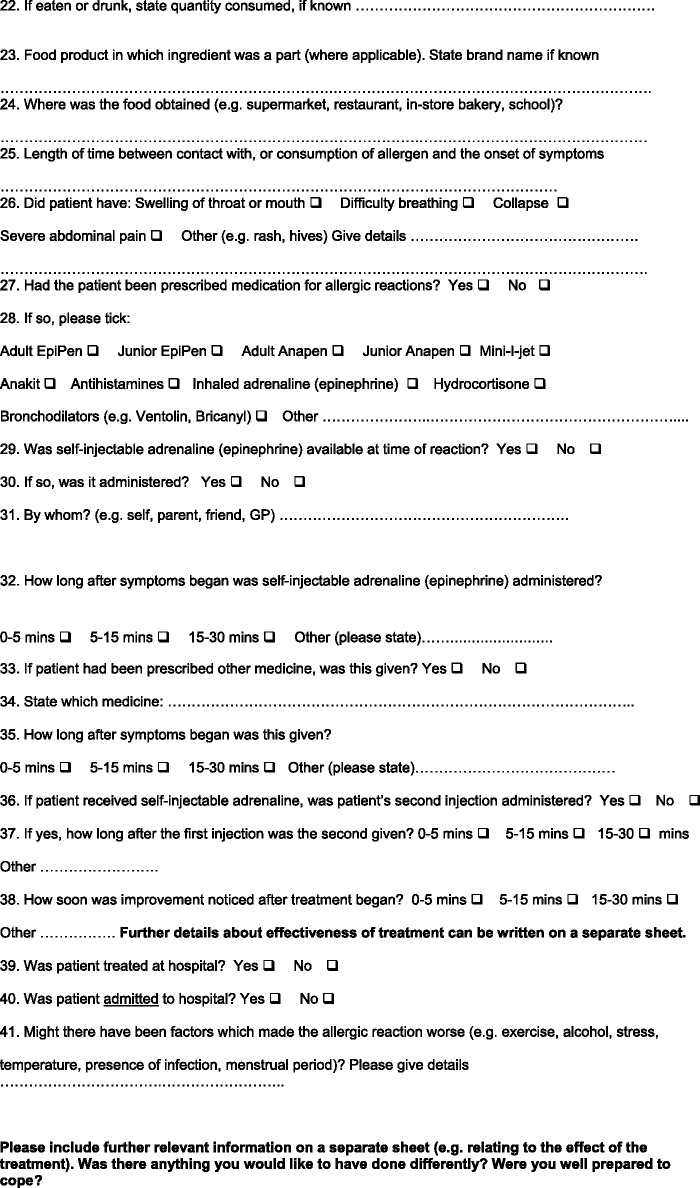
Self-completed questionnaire.
The age of participants ranged from 0 to 72 years.
We analysed data from self-completed questionnaires collected over a 12-year period, i.e. 2001-2013, available to people by phone and, since 2012, for online completion through the Anaphylaxis Campaign.
We analysed data from self-completed questionnaires collected over a 12- year period, i.e. 2001-2013, available to people by phone and, since 2012, for online completion through the Anaphylaxis Campaign.
In total, 356 questionnaires were submitted, of which 54 did not meet the criteria for anaphylaxis. The remaining 302 anaphylactic reactions originated from 243 individuals; 193 (64%) of these reactions were in children. Approximately half of all reactions occurred at home ( = 148; 49%); 61% ( = 193) of reactions occurred in those reporting a history of asthma, and many ( = 76; 41%) of these individuals had asthma that they classified as being severe. In 57% ( = 173) cases, the respondent reacted to a known allergen. Self-injectable adrenaline (epinephrine) was available in 79% of the cases, and it was only used in 38% of episodes. The usage of self-injected adrenaline was lower in children (30%) than in adults (54%), even though 82% of children had adrenaline available at the time of the reaction compared to 74% of adults.
These data suggest that the majority of anaphylaxis reactions are triggered by exposure to known food allergens and that approximately half of these reactions occur at home. Access to self-injectable adrenaline was sub-optimal and when available it was only used in a minority of cases. Avoiding triggers, access to self-injectable adrenaline and its prompt use in the context of reactions need to be reinforced.
研究儿童和成人过敏反应的情况、特征及处理方法。
自行填写的问卷。
参与者年龄范围为0至72岁。
我们分析了在12年期间(即2001年至2013年)收集的自行填写问卷的数据,这些问卷可通过电话获取,自2012年起也可通过过敏反应运动在线填写。
我们分析了在12年期间(即2001年至2013年)收集的自行填写问卷的数据,这些问卷可通过电话获取,自2012年起也可通过过敏反应运动在线填写。
共提交了356份问卷,其中54份不符合过敏反应标准。其余302例过敏反应来自243人;其中193例(64%)反应发生在儿童身上。所有反应中约一半发生在家中(=148;49%);61%(=193)的反应发生在有哮喘病史的人身上,其中许多人(=76;41%)将自己的哮喘归类为重度。在57%(=173)的病例中,受访者对已知过敏原产生反应。79%的病例备有自动注射肾上腺素,而仅在38%的发作中使用。儿童自动注射肾上腺素的使用率(30%)低于成人(54%),尽管反应发生时82%的儿童备有肾上腺素,而成人这一比例为74%。
这些数据表明,大多数过敏反应是由接触已知食物过敏原引发的,且这些反应约一半发生在家中。自动注射肾上腺素的可及性欠佳,即便有药,也仅在少数病例中使用。需要加强避免接触过敏原、获取自动注射肾上腺素以及在反应发生时及时使用的措施。