Herrington William, Staplin Natalie, Judge Parminder K, Mafham Marion, Emberson Jonathan, Haynes Richard, Wheeler David C, Walker Robert, Tomson Charlie, Agodoa Larry, Wiecek Andrzej, Lewington Sarah, Reith Christina A, Landray Martin J, Baigent Colin
From the Clinical Trial Service Unit and Epidemiological Studies Unit (CTSU), (W.H., N.S., P.K.J., M.M., J.E., R.H., S.L., C.A.R., M.J.L., C.B.) and Medical Research Council-Population Health Research Unit (MRC-PHRU) (P.K.J., J.E., R.H., S.L., C.B.), Nuffield Department of Population Health (NDPH), University of Oxford, United Kingdom; Centre for Nephrology, University College London, United Kingdom (D.C.W.); Dunedin School of Medicine, University of Otago, New Zealand (R.W.); Newcastle-upon-Tyne Hospitals NHS Foundation Trust, United Kingdom (C.T.); National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, MD (L.A.); and Department of Nephrology, Transplantation and Internal Medicine, Medical University of Silesia, Katowice, Poland (A.W.).
Hypertension. 2017 Feb;69(2):314-322. doi: 10.1161/HYPERTENSIONAHA.116.08386. Epub 2016 Dec 27.
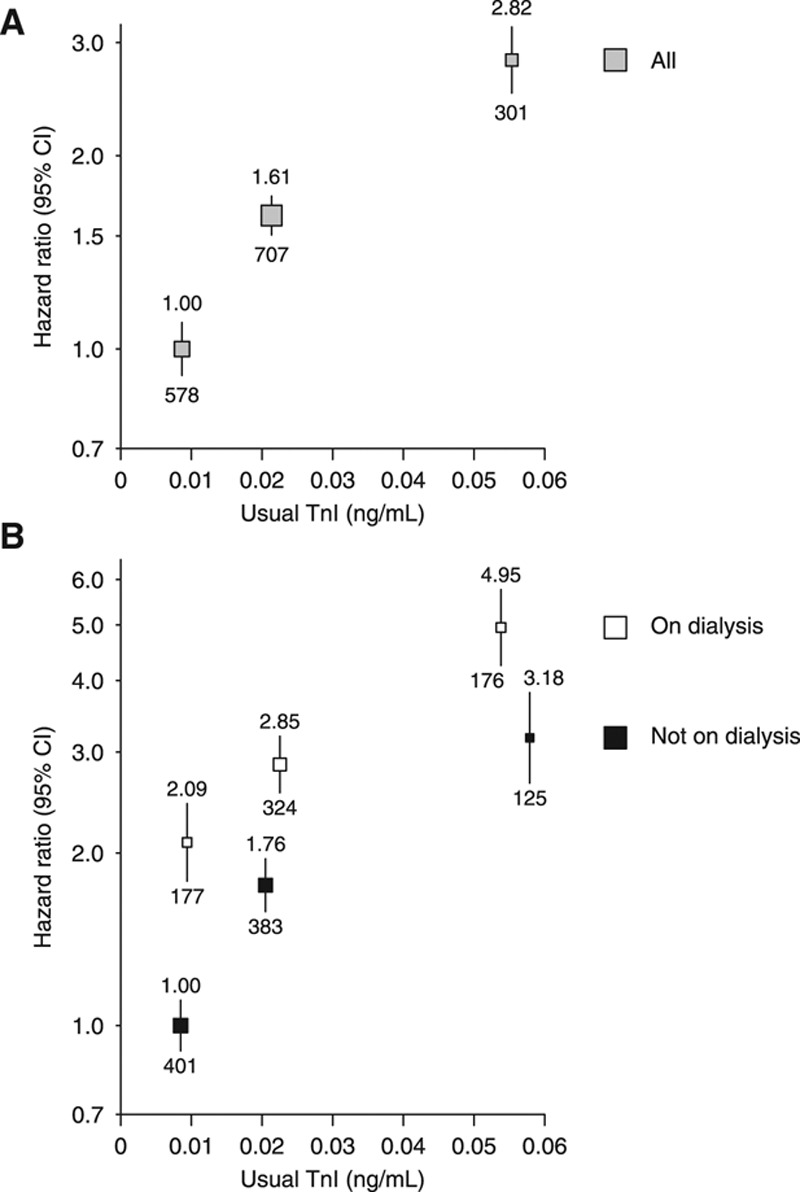
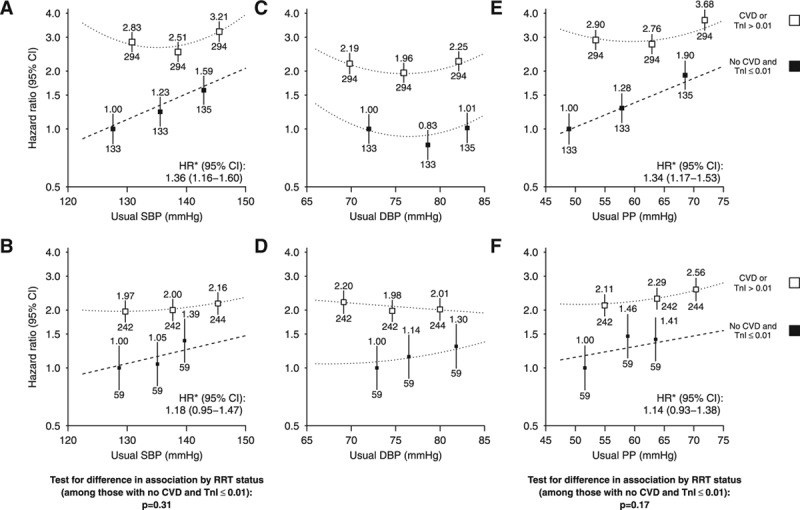
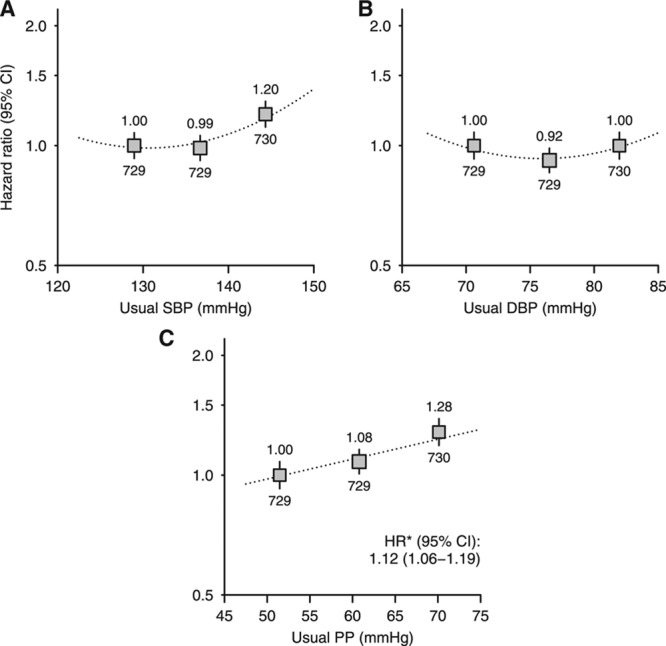
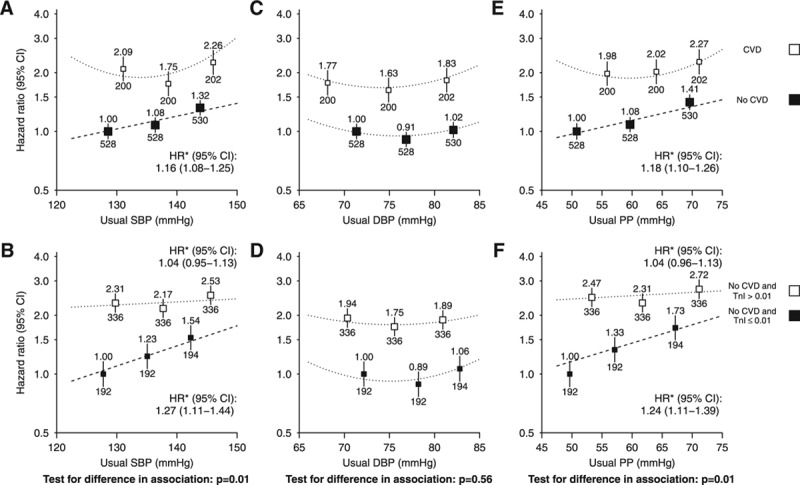
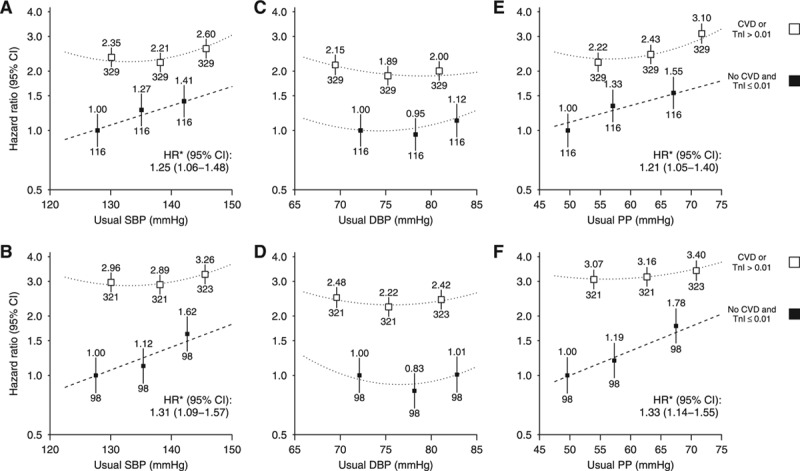
Among those with moderate-to-advanced chronic kidney disease, the relationship between blood pressure (BP) and cardiovascular disease seems U shaped but is loglinear in apparently healthy adults. The SHARP (Study of Heart and Renal Protection) randomized 9270 patients with chronic kidney disease to ezetimibe/simvastatin versus matching placebo and measured BP at each follow-up visit. Cox regression was used to assess the association between BP and risk of cardiovascular disease among (1) those with a self-reported history of cardiovascular disease and (2) those with no such history and, based on plasma troponin-I concentration, a low probability of subclinical cardiac disease. A total of 8666 participants had a valid baseline BP and troponin-I measurement, and 2188 had at least 1 cardiovascular event during follow-up. After adjustment for relevant confounders, the association between systolic BP and cardiovascular events was U shaped, but among participants without evidence of previous cardiovascular disease, there was a positive loglinear association throughout the range of values studied. Among those with the lowest probability of subclinical cardiac disease, each 10 mm Hg higher systolic BP corresponded to a 27% increased risk of cardiovascular disease (hazard ratio, 1.27; 95% confidence interval, 1.11-1.44). In contrast, the relationship between diastolic BP and cardiovascular risk remained U shaped irrespective of cardiovascular disease history or risk of subclinical disease. In conclusion, the lack of a clear association between systolic BP and cardiovascular risk in this population seems attributable to confounding, suggesting that more intensive systolic BP reduction may be beneficial in such patients.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT00125593.
在中重度慢性肾脏病患者中,血压(BP)与心血管疾病之间的关系似乎呈U形,但在明显健康的成年人中呈对数线性关系。心脏和肾脏保护研究(SHARP)将9270例慢性肾脏病患者随机分为依折麦布/辛伐他汀组和匹配的安慰剂组,并在每次随访时测量血压。采用Cox回归评估(1)有心血管疾病自我报告史的患者和(2)无此类病史且根据血浆肌钙蛋白I浓度判断亚临床心脏病可能性低的患者中,血压与心血管疾病风险之间的关联。共有8666名参与者进行了有效的基线血压和肌钙蛋白I测量,2188名参与者在随访期间至少发生1次心血管事件。在调整相关混杂因素后,收缩压与心血管事件之间的关联呈U形,但在无既往心血管疾病证据的参与者中,在所研究的整个血压值范围内存在正对数线性关联。在亚临床心脏病可能性最低的患者中,收缩压每升高10 mmHg,心血管疾病风险增加27%(风险比,1.27;95%置信区间,1.11 - 1.44)。相比之下,舒张压与心血管风险之间的关系无论心血管疾病史或亚临床疾病风险如何均保持U形。总之,该人群中收缩压与心血管风险之间缺乏明确关联似乎归因于混杂因素,这表明更积极地降低收缩压可能对此类患者有益。