Vergis Nikhil, Atkinson Stephen R, Knapp Suzanne, Maurice James, Allison Michael, Austin Andrew, Forrest Ewan H, Masson Steven, McCune Anne, Patch David, Richardson Paul, Gleeson Dermot, Ryder Stephen D, Wright Mark, Thursz Mark R
Imperial College, London, United Kingdom.
Imperial College, London, United Kingdom.
Gastroenterology. 2017 Apr;152(5):1068-1077.e4. doi: 10.1053/j.gastro.2016.12.019. Epub 2016 Dec 30.
BACKGROUND & AIMS: Infections are common in patients with severe alcoholic hepatitis (SAH), but little information is available on how to predict their development or their effects on patients. Prednisolone is advocated for treatment of SAH, but can increase susceptibility to infection. We compared the effects of infection on clinical outcomes of patients treated with and without prednisolone, and identified risk factors for development of infection in SAH.
We analyzed data from 1092 patients enrolled in a double-blind placebo-controlled trial to evaluate the efficacy of treatment with prednisolone (40 mg daily) or pentoxifylline (400 mg 3 times each day) in patients with SAH. The 2 × 2 factorial design led to 547 patients receiving prednisolone; 546 were treated with pentoxifylline. The trial was conducted in the United Kingdom from January 2011 through February 2014. Data on development of infection were collected at evaluations performed at screening, baseline, weekly during admission, on discharge, and after 90 days. Patients were diagnosed with infection based on published clinical and microbiologic criteria. Risk factors for development of infection and effects on 90-day mortality were evaluated separately in patients treated with prednisolone (n = 547) and patients not treated with prednisolone (n = 545) using logistic regression. Pretreatment blood levels of bacterial DNA (bDNA) were measured in 731 patients.
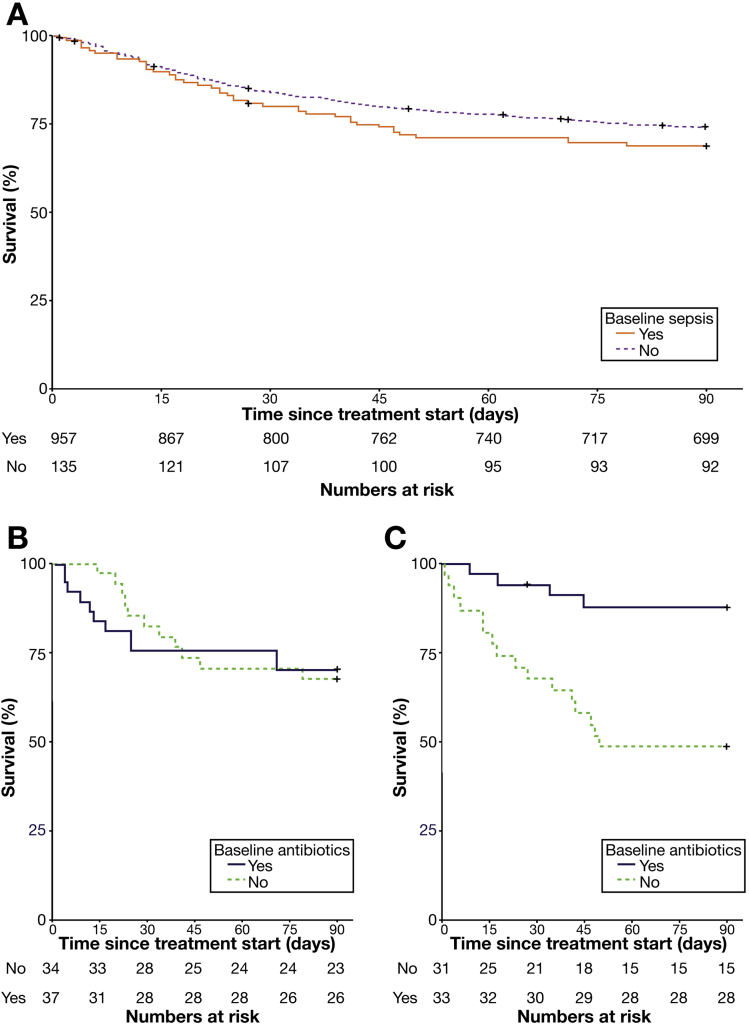
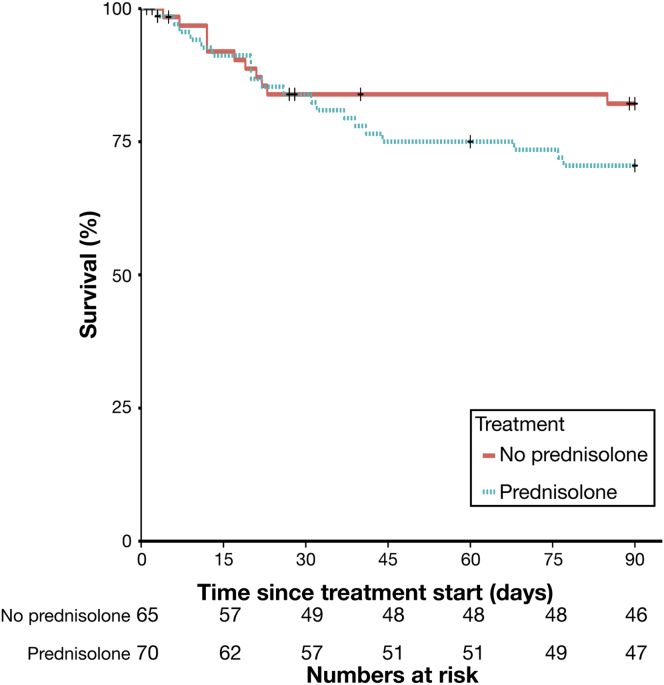
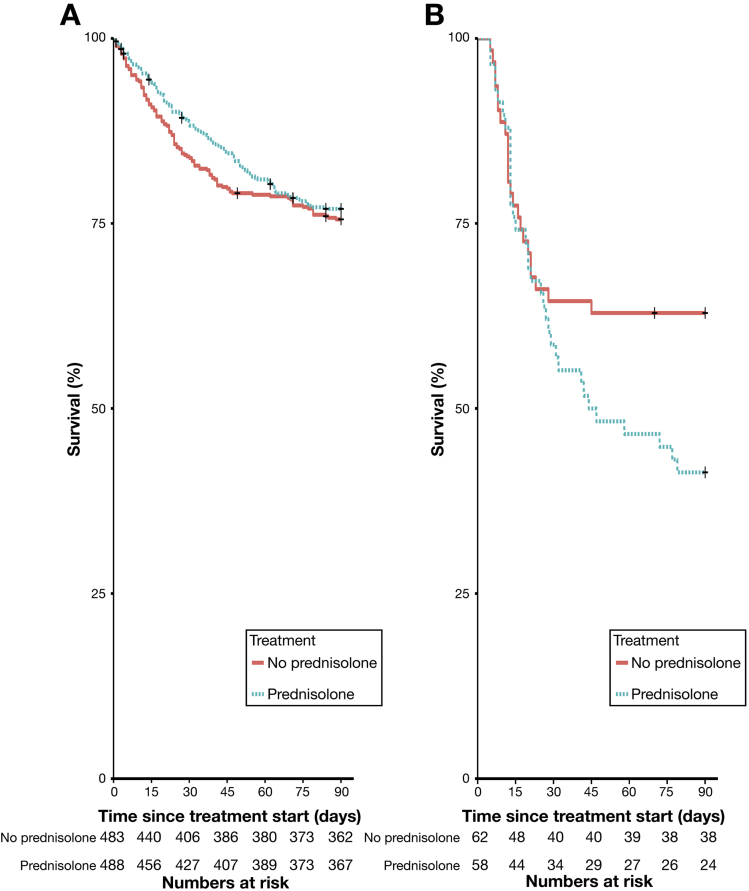
Of the 1092 patients in the study, 135 had an infection at baseline, 251 developed infections during treatment, and 89 patients developed an infection after treatment. There was no association between pentoxifylline therapy and the risk of serious infection (P = .084), infection during treatment (P = .20), or infection after treatment (P = .27). Infections classified as serious were more frequent in patients treated with prednisolone (odds ratio [OR], 1.27; 95% confidence interval [CI], 1.27-2.92; P = .002). There was no association between prednisolone therapy and infection during treatment (OR, 1.04; 95% CI, 0.78-1.37; P = .80). However, a higher proportion (10%) of patients receiving prednisolone developed an infection after treatment than of patients not given prednisolone (6%) (OR, 1.70; 95% CI, 1.07-2.69; P = .024). Development of infection was associated with increased 90-day mortality in patients with SAH treated with prednisolone, independent of model for end-stage liver disease or Lille score (OR, 2.46; 95% CI, 1.41-4.30; P = .002). High circulating bDNA predicted infection that developed within 7 days of prednisolone therapy, independent of Model for End-Stage Liver Disease and white blood cell count (OR, 4.68; 95% CI, 1.80-12.17; P = .001). In patients who did not receive prednisolone, infection was not independently associated with 90-day mortality (OR, 0.94; 95% CI, 0.54-1.62; P = .82) or levels of bDNA (OR, 0.83; 95% CI, 0.39-1.75; P = .62).
Patients with SAH given prednisolone are at greater risk for developing serious infections and infections after treatment than patients not given prednisolone, which may offset its therapeutic benefit. Level of circulating bDNA before treatment could identify patients at high risk of infection if given prednisolone; these data could be used to select therapies for patients with SAH. EudraCT no: 2009-013897-42; Current Controlled Trials no: ISRCTN88782125.
感染在重症酒精性肝炎(SAH)患者中很常见,但关于如何预测感染的发生及其对患者的影响,目前可用信息较少。泼尼松龙被推荐用于治疗SAH,但会增加感染易感性。我们比较了感染对接受和未接受泼尼松龙治疗患者临床结局的影响,并确定了SAH患者感染发生的危险因素。
我们分析了1092例参加双盲安慰剂对照试验患者的数据,以评估泼尼松龙(每日40mg)或己酮可可碱(每次400mg,每日3次)治疗SAH患者的疗效。2×2析因设计导致547例患者接受泼尼松龙治疗;546例接受己酮可可碱治疗。该试验于2011年1月至2014年2月在英国进行。在筛查、基线、入院期间每周、出院时及90天后的评估中收集感染发生的数据。根据已发表的临床和微生物学标准诊断患者是否感染。使用逻辑回归分别评估接受泼尼松龙治疗的患者(n = 547)和未接受泼尼松龙治疗的患者(n = 545)中感染发生的危险因素及其对90天死亡率的影响。在731例患者中检测了治疗前血液中细菌DNA(bDNA)水平。
在该研究的1092例患者中,135例在基线时感染,251例在治疗期间发生感染,89例在治疗后发生感染。己酮可可碱治疗与严重感染风险(P = 0.084)、治疗期间感染(P = 0.20)或治疗后感染(P = 0.27)之间无关联。在接受泼尼松龙治疗的患者中,严重感染更为常见(比值比[OR],1.27;95%置信区间[CI],1.27 - 2.92;P = 0.002)。泼尼松龙治疗与治疗期间感染之间无关联(OR,1.04;95%CI,0.78 - 1.37;P = 0.80)。然而,接受泼尼松龙治疗的患者中,治疗后发生感染的比例(10%)高于未接受泼尼松龙治疗的患者(6%)(OR,1.70;95%CI,1.07 - 2.69;P = 0.024)。感染的发生与接受泼尼松龙治疗的SAH患者90天死亡率增加相关,与终末期肝病模型或里尔评分无关(OR,2.46;95%CI,1.41 - 4.30;P = 0.002)。高循环bDNA可预测泼尼松龙治疗7天内发生的感染,与终末期肝病模型和白细胞计数无关(OR,4.68;95%CI,1.80 - 12.17;P = 0.001)。在未接受泼尼松龙治疗的患者中,感染与90天死亡率(OR,0.94;95%CI,0.54 - 1.62;P = 0.82)或bDNA水平(OR,0.83;95%CI,0.39 - 1.75;P = 0.62)无独立关联。
与未接受泼尼松龙治疗的患者相比,接受泼尼松龙治疗的SAH患者发生严重感染和治疗后感染的风险更高,这可能抵消其治疗益处。治疗前循环bDNA水平可识别接受泼尼松龙治疗时感染高危患者;这些数据可用于为SAH患者选择治疗方法。欧洲临床试验注册号:2009 - 013897 - 42;当前受控试验注册号:ISRCTN88782125。