Pelz Johann Otto, Weinreich Anna, Karlas Thomas, Saur Dorothee
Department of Neurology, Leipzig University Hospital, Leipzig, Germany.
Department of Gastroenterology and Rheumatology, Leipzig University Hospital, Leipzig, Germany.
PLoS One. 2017 Jan 3;12(1):e0167500. doi: 10.1371/journal.pone.0167500. eCollection 2017.
Currently, colour-coded duplex sonography (2D-CDS) is clinical standard for detection and grading of internal carotid artery stenosis (ICAS). However, unlike angiographic imaging modalities, 2D-CDS assesses ICAS by its hemodynamic effects rather than luminal changes. Aim of this study was to evaluate freehand 3D ultrasound (3DUS) for direct visualisation and quantification of ICAS.
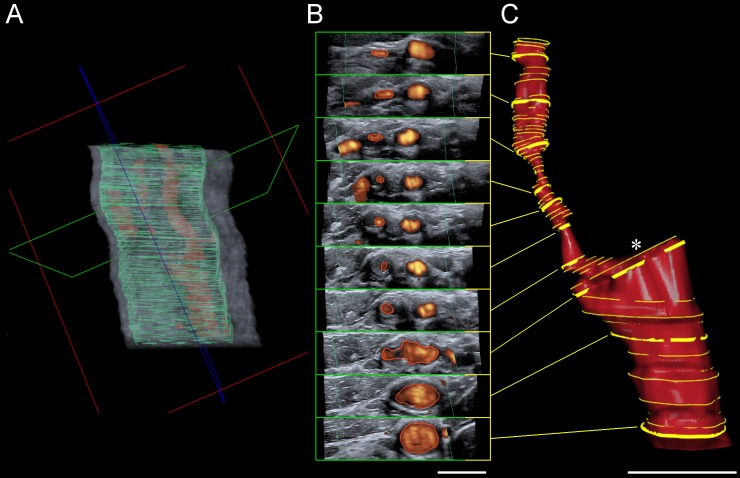
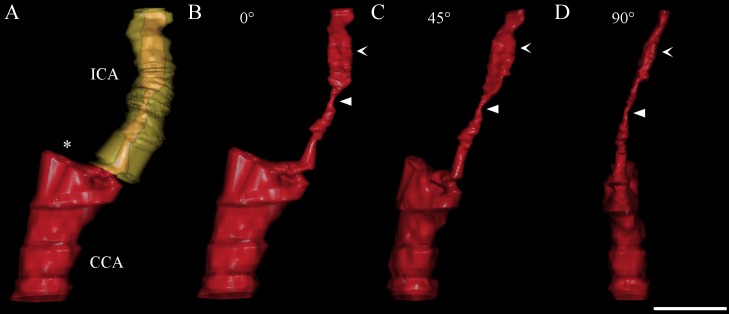
Thirty-seven patients with 43 ICAS were examined with 2D-CDS as reference standard and with freehand B-mode respectively power-mode 3DUS. Stenotic value of 3D reconstructed ICAS was calculated as distal diameter respectively distal cross-sectional area (CSA) reduction percentage and compared with 2D-CDS.
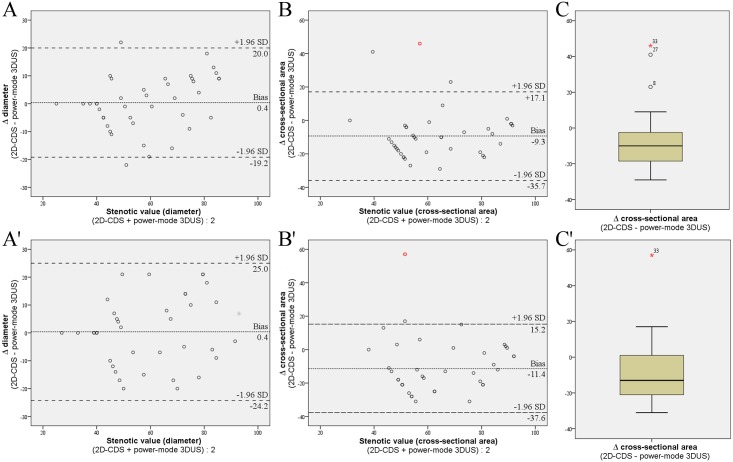
There was a trend but no significant difference in successful 3D reconstruction of ICAS between B-mode and power mode (examiner 1 {Ex1} 81% versus 93%, examiner 2 {Ex2} 84% versus 88%). Inter-rater agreement was best for power-mode 3DUS and assessment of stenotic value as distal CSA reduction percentage (intraclass correlation coefficient {ICC} 0.90) followed by power-mode 3DUS and distal diameter reduction percentage (ICC 0.81). Inter-rater agreement was poor for B-mode 3DUS (ICC, distal CSA reduction 0.36, distal diameter reduction 0.51). Intra-rater agreement for power-mode 3DUS was good for both measuring methods (ICC, distal CSA reduction 0.88 {Ex1} and 0.78 {Ex2}; ICC, distal diameter reduction 0.83 {Ex1} and 0.76 {Ex2}). In comparison to 2D-CDS inter-method agreement was good and clearly better for power-mode 3DUS (ICC, distal diameter reduction percentage: Ex1 0.85, Ex2 0.78; distal CSA reduction percentage: Ex1 0.63, Ex2 0.57) than for B-mode 3DUS (ICC, distal diameter reduction percentage: Ex1 0.40, Ex2 0.52; distal CSA reduction percentage: Ex1 0.15, Ex2 0.51).
Non-invasive power-mode 3DUS is superior to B-mode 3DUS for imaging and quantification of ICAS. Thereby, further studies are warranted which should now compare power-mode 3DUS with the angiographic gold standard imaging modalities for quantification of ICAS, i.e. with CTA or CE-MRA.
目前,彩色编码双功超声检查(2D-CDS)是检测和分级颈内动脉狭窄(ICAS)的临床标准。然而,与血管造影成像方式不同,2D-CDS通过其血流动力学效应而非管腔变化来评估ICAS。本研究的目的是评估徒手三维超声(3DUS)用于直接可视化和量化ICAS。
以2D-CDS作为参考标准,对37例患有43处ICAS的患者分别进行徒手B模式或能量模式3DUS检查。3D重建ICAS的狭窄值计算为远端直径或远端横截面积(CSA)减少百分比,并与2D-CDS进行比较。
B模式和能量模式在ICAS的成功3D重建方面有一定趋势,但无显著差异(检查者1{Ex1}为81%对93%,检查者2{Ex2}为84%对88%)。评分者间一致性在能量模式3DUS以及将狭窄值评估为远端CSA减少百分比时最佳(组内相关系数{ICC}为0.90),其次是能量模式3DUS和远端直径减少百分比(ICC为0.81)。B模式3DUS的评分者间一致性较差(ICC,远端CSA减少为0.36,远端直径减少为0.51)。能量模式3DUS的评分者内一致性在两种测量方法中均良好(ICC,远端CSA减少:Ex1为0.88,Ex2为0.78;ICC,远端直径减少:Ex1为0.83,Ex2为0.76)。与2D-CDS相比, 方法间一致性良好,能量模式三维超声明显优于B模式三维超声(ICC,远端直径减少百分比:Ex1为0.85,Ex2为0.78;远端CSA减少百分比:Ex1为0.63,Ex2为0.57),而B模式三维超声(ICC,远端直径减少百分比:Ex1为0.40,Ex2为0.52;远端CSA减少百分比:Ex1为0.15,Ex2为0.51)。
无创能量模式3DUS在ICAS成像和量化方面优于B模式3DUS。因此,有必要进行进一步研究,现在应将能量模式3DUS与用于ICAS量化的血管造影金标准成像方式,即CTA或CE-MRA进行比较。