Okello Emmy, Longenecker Chris T, Beaton Andrea, Kamya Moses R, Lwabi Peter
Uganda Heart Institute, Kampala, Uganda.
Department of Medicine, School of Medicine Makerere University, Kampala, Uganda.
BMC Cardiovasc Disord. 2017 Jan 7;17(1):20. doi: 10.1186/s12872-016-0451-8.
Rheumatic heart disease (RHD), the long-term consequence of rheumatic fever, accounts for most cardiovascular morbidity and mortality among young adults in developing countries. However, data on contemporary outcomes from resource constrained areas are limited.
A prospective cohort study of participants aged 5-60 years with established RHD was conducted in Kampala, Uganda, in which clinical exam, echocardiography, electrocardiography (ECG), and laboratory evaluation were done every 3 months and every 4-week benzathine penicillin prophylaxis was prescribed. Participants were followed up for 12 months and outcomes and predictors of morbidity and mortality were assessed using Kaplan Meier curves and Cox proportional hazards models.
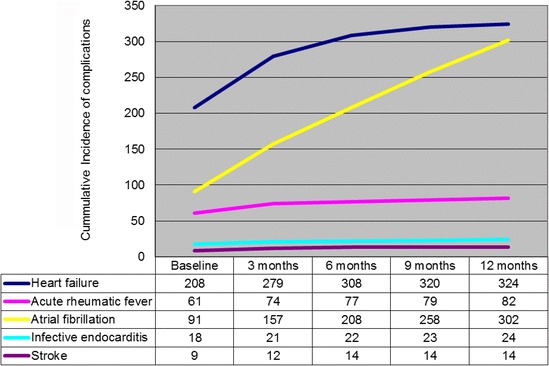
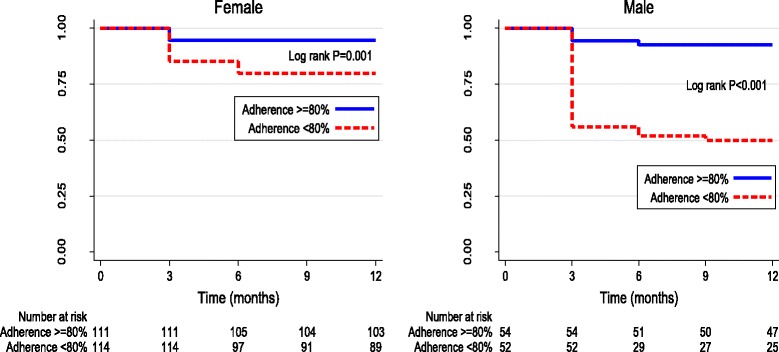
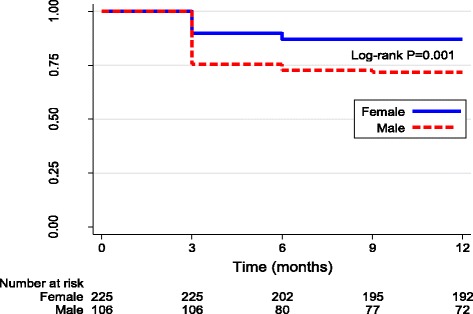
Of 449 subjects, 66.8% (300/449) were females, median age was 30 (interquartile range 20). 73.7% (331/449) had atleast one follow up visit. Among these, 35% (116/331) developed decompensated heart failure and, 63.7% (211/331) developed atrial fibrillation. Heart failure was associated with poor penicillin adherence (OR = 3.3, CI 2-5.4, p = 0.001), and left ventricular end diastolic diameter greater than 55 mm (OR = 3.16, CI 1.73-5.76, p = 0.001). Atrial fibrillation was associated with left atrial diameter >40 mm (OR = 7.5, CI 2.4-9.8, p = 0.001). There were 59 deaths with a 1-year mortality rate of 17.8%. Most deaths occurred within the first three months of presentation. Subjects whose average adherence to benzathine penicillin was <80% had significantly greater mortality (31% vs. 9%, log rank p < 0.001). In multivariate analysis, the risk of death among those with poor penicillin adherence was 3.81 times higher than those with better adherence (HR = 3.81, CI 1.92-7.63, p = 0.001). Other predictors of 1 year mortality included heart failure (HR 8.36, CI 3.28-21.31, p = 0.001) and left ventricular end diastolic diameter greater than 55 mm (HR = 1.93, CI 1.07-3.49, p = 0.02).
In this study of RHD in Uganda, morbidity and mortality within 1 year of presentation were higher than in recently published from other low and middle income countries. Suboptimal adherence to benzathine penicillin injections was associated with incident heart failure and mortality over 1 year. Future studies should test interventions to improve adherence among patients with advanced disease who are at the highest risk of mortality.
风湿性心脏病(RHD)是风湿热的长期后果,在发展中国家的年轻成年人中占大多数心血管疾病的发病率和死亡率。然而,来自资源有限地区的当代结局数据有限。
在乌干达坎帕拉对5至60岁确诊为RHD的参与者进行了一项前瞻性队列研究,每3个月进行一次临床检查、超声心动图、心电图(ECG)和实验室评估,并每4周开具苄星青霉素预防性用药。对参与者进行了12个月的随访,并使用Kaplan Meier曲线和Cox比例风险模型评估发病率和死亡率的结局及预测因素。
在449名受试者中,66.8%(300/449)为女性,中位年龄为30岁(四分位间距20)。73.7%(331/449)至少有一次随访。其中,35%(116/331)发生失代偿性心力衰竭,63.7%(211/331)发生心房颤动。心力衰竭与苄星青霉素依从性差相关(OR = 3.3,CI 2 - 5.4,p = 0.001),以及左心室舒张末期直径大于55mm(OR = 3.16,CI 1.73 - 5.76,p = 0.001)。心房颤动与左心房直径>40mm相关(OR = 7.5,CI 2.4 - 9.8,p = 0.001)。有59例死亡,1年死亡率为17.8%。大多数死亡发生在就诊后的前三个月内。苄星青霉素平均依从性<80%的受试者死亡率显著更高(31%对9%,对数秩检验p < 0.001)。在多变量分析中,苄星青霉素依从性差的患者死亡风险比依从性好的患者高3.81倍(HR = 3.81,CI 1.92 - 7.63,p = 0.001)。1年死亡率的其他预测因素包括心力衰竭(HR 8.36,CI 3.28 - 21.31,p = 0.001)和左心室舒张末期直径大于55mm(HR = 1.93,CI 1.07 - 3.49,p = 0.02)。
在这项乌干达RHD研究中,就诊后1年内的发病率和死亡率高于最近其他低收入和中等收入国家公布的数据。苄星青霉素注射的依从性欠佳与1年内发生心力衰竭和死亡相关。未来的研究应测试干预措施,以提高处于最高死亡风险的晚期疾病患者的依从性。