Dasgupta Kaberi, Rosenberg Ellen, Joseph Lawrence, Cooke Alexandra B, Trudeau Luc, Bacon Simon L, Chan Deborah, Sherman Mark, Rabasa-Lhoret Rémi, Daskalopoulou Stella S
Division of Clinical Epidemiology, Department of Medicine, McGill University Health Centre, Montréal, Québec, Canada.
Division of Endocrinology, McGill University, Montreal, Québec, Canada.
Diabetes Obes Metab. 2017 May;19(5):695-704. doi: 10.1111/dom.12874. Epub 2017 Feb 22.
There are few proven strategies to enhance physical activity and cardiometabolic profiles in patients with type 2 diabetes and hypertension. We examined the effects of physician-delivered step count prescriptions and monitoring.
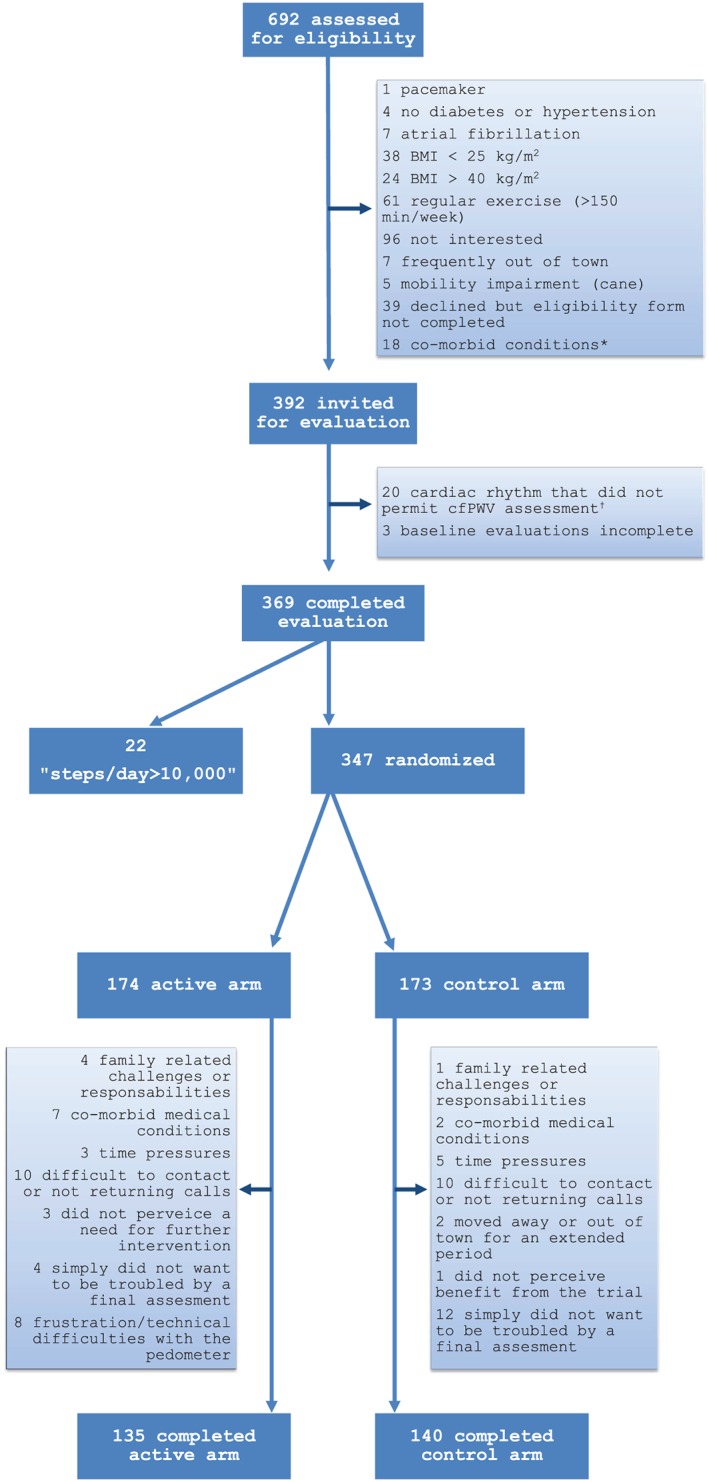
Participants randomized to the active arm were provided with pedometers and they recorded step counts. Over a 1-year period, their physicians reviewed their records and provided a written step count prescription at each clinic visit. The overall goal was a 3000 steps/day increase over 1 year (individualized rate of increase). Control arm participants were advised to engage in physical activity 30 to 60 min/day. We evaluated effects on step counts, carotid femoral pulse wave velocity (cfPWV, primary) and other cardiometabolic indicators including haemoglobin A1c in diabetes (henceforth abbreviated as A1c) and Homeostasis Model Assessment-Insulin Resistance (HOMA-IR) in participants not receiving insulin therapy.
A total of 79% completed final evaluations (275/347; mean age, 60 years; SD, 11). Over 66% of participants had type 2 diabetes and over 90% had hypertension. There was a net 20% increase in steps/day in active vs control arm participants (1190; 95% CI, 550-1840). Changes in cfPWV were inconclusive; active vs control arm participants with type 2 diabetes experienced a decrease in A1c (-0.38%; 95% CI, -0.69 to -0.06). HOMA-IR also declined in the active arm vs the control arm (ie, assessed in all participants not treated with insulin; -0.96; 95% CI, -1.72 to -0.21).
A simple physician-delivered step count prescription strategy incorporated into routine clinical practice led to a net 20% increase in step counts; however, this was below the 3000 steps/day targeted increment. While conclusive effects on cfPWV were not observed, there were improvements in both A1c and insulin sensitivity. Future studies will evaluate an amplified intervention to increase impact.
在2型糖尿病和高血压患者中,几乎没有经过验证的策略可增强身体活动及改善心脏代谢指标。我们研究了医生提供的步数处方及监测的效果。
随机分配至干预组的参与者被提供了计步器并记录步数。在1年的时间里,他们的医生查看记录,并在每次门诊就诊时提供书面步数处方。总体目标是1年内每天增加3000步(个性化增加速率)。对照组参与者被建议每天进行30至60分钟的身体活动。我们评估了对步数、颈股脉搏波速度(cfPWV,主要指标)以及其他心脏代谢指标的影响,这些指标包括糖尿病患者的糖化血红蛋白(此后简称为A1c)以及未接受胰岛素治疗参与者的稳态模型评估胰岛素抵抗(HOMA-IR)。
共有79%的参与者完成了最终评估(275/347;平均年龄60岁;标准差11)。超过66%的参与者患有2型糖尿病,超过90%的参与者患有高血压。干预组参与者每天的步数净增加20%(1190步;95%置信区间,550 - 1840步)。cfPWV的变化尚无定论;2型糖尿病的干预组参与者与对照组参与者相比,A1c有所下降(-0.38%;95%置信区间,-0.69至-0.06)。与对照组相比,干预组的HOMA-IR也有所下降(即,在所有未接受胰岛素治疗的参与者中进行评估;-0.96;95%置信区间,-1.72至-0.21)。
纳入常规临床实践的简单的医生提供的步数处方策略使步数净增加了20%;然而,这低于每天增加3000步的目标增量。虽然未观察到对cfPWV的确切影响,但A1c和胰岛素敏感性均有所改善。未来的研究将评估强化干预措施以增强效果。