Cai Zhengyi, Li Huijing, Wang Xun, Niu Xiaoting, Ni Peiqi, Zhang Wanli, Shao Bei
aDepartment of Neurology bDepartment of Pediatrics, First Affiliated Hospital of Wenzhou Medical University, Wenzhou, Zhejiang Province, China.
Medicine (Baltimore). 2017 Jan;96(2):e5898. doi: 10.1097/MD.0000000000005898.
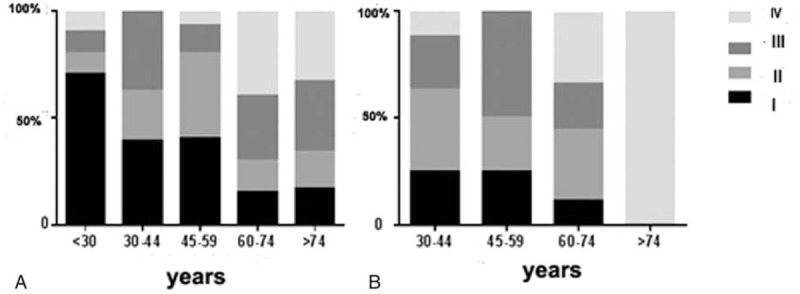
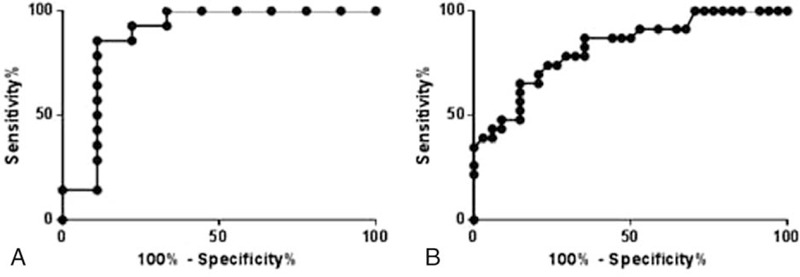
The aim of this study was to compare clinical characteristics, electroneurography (ENoG) results, and functional outcomes of patients with Bell's palsy (BP) and Ramsay Hunt syndrome (RHS).Around 57 patients with BP and 23 patients with RHS were enrolled in this study from January 2010 and September 2015. Both clinical characteristics and ENoG results were recorded at hospital admission. The evaluations of functional outcomes were conducted with House-Brackmann (H-B) grading system at 6-month follow-up.There were no significant differences in age, gender proportion, initial H-B grades, time before commencement of treatment and the presence of comorbid disease in 2 groups. However, the final H-B grades at 6-month follow-up were significantly better in BP patients than RHS patients. The results of ENoG showed that degeneration index (DI) was significantly higher in the RHS group than the BP group. But no significant difference was found in the value of prolonged latency time (PLT) between the 2 groups. In multivariate analysis, age and ENoG DI were independently associated with functional outcome of recovery in the BP group (OR 0.167, 95% CI 0.038-0.622, P = 0.009 and OR 0.289 95% CI 0.107-0.998, P = 0.050, respectively). However, in the RHS group, only ENoG DI was related to the final H-B grades (OR 0.067, 95% CI 0.005-0.882, P = 0.040). Spearman's rank correlation analysis showed that higher age and ENoG DI were related to poorer prognosis in 2 groups (P < 0.05). PLT was related to functional outcomes only in the BP group (rs = 0.460, P < 0.001). The receiver operating characteristic (ROC) of ENoG DI analysis revealed that the cutoff value was 67.0% for BP prognosis and 64.5% for RHS prognosis. What's more, patients with hypertension or diabetes mellitus had both higher final H-B grade and ENoG DI than those without the same comorbidity.Patients with RHS had poorer prognosis than those with BP. Some factors including age, ENoG DI, and the presence of disease influenced recovery from BP and RHS. The present study demonstrated that BP patients with ENoG DI < 67.0% and RHS patients with ENoG DI < 65.5% had a greater opportunity for recovery within half a year.
本研究旨在比较贝尔麻痹(BP)和拉姆齐·亨特综合征(RHS)患者的临床特征、神经电生理检查(ENoG)结果及功能预后。2010年1月至2015年9月,本研究纳入了约57例BP患者和23例RHS患者。入院时记录临床特征及ENoG结果。在6个月随访时采用House-Brackmann(H-B)分级系统对功能预后进行评估。两组患者在年龄、性别比例、初始H-B分级、治疗开始前时间及合并疾病方面无显著差异。然而,BP患者6个月随访时的最终H-B分级显著优于RHS患者。ENoG结果显示,RHS组的变性指数(DI)显著高于BP组。但两组间的延长潜伏期时间(PLT)值无显著差异。多因素分析显示,年龄和ENoG DI与BP组的恢复功能预后独立相关(OR分别为0.167,95%CI为0.038 - 0.622,P = 0.009;OR为0.289,95%CI为0.107 - 0.998,P = 0.050)。然而,在RHS组,仅ENoG DI与最终H-B分级相关(OR为0.067,95%CI为0.005 - 0.882,P = 0.040)。Spearman等级相关分析显示,年龄越大和ENoG DI越高与两组预后越差相关(P < 0.05)。PLT仅与BP组的功能预后相关(rs = 0.460,P < 0.001)。ENoG DI分析的受试者工作特征(ROC)曲线显示,BP预后的截断值为67.0%,RHS预后的截断值为64.5%。此外,高血压或糖尿病患者的最终H-B分级及ENoG DI均高于无相同合并症的患者。RHS患者的预后比BP患者差。年龄、ENoG DI及疾病存在等一些因素影响BP和RHS的恢复。本研究表明,ENoG DI < 67.0%的BP患者和ENoG DI < 65.5%的RHS患者在半年内恢复的机会更大。