Rebnord Ingrid Keilegavlen, Sandvik Hogne, Mjelle Anders Batman, Hunskaar Steinar
National Centre for Emergency Primary Health Care, Uni Research Health, Bergen, Norway.
Department of Global Public Health and Primary Care, University of Bergen, Bergen, Norway.
BMJ Open. 2017 Jan 17;7(1):e012992. doi: 10.1136/bmjopen-2016-012992.
Acute respiratory infections and fever among children are highly prevalent in primary care. It is challenging to distinguish between viral and bacterial infections. Norway has a relatively low prescription rate of antibiotics, but it is still regarded as too high as the antimicrobial resistance is increasing. The aim of the study was to identify predictors for prescribing antibiotics or referral to hospital among children.
Secondary analysis of a randomised controlled study.
4 out-of-hours services and 1 paediatric emergency clinic in Norwegian primary care.
401 children aged 0-6 years with respiratory symptoms and/or fever visiting the out-of-hours services.
2 main outcome variables were registered: antibiotic prescription and referral to hospital.
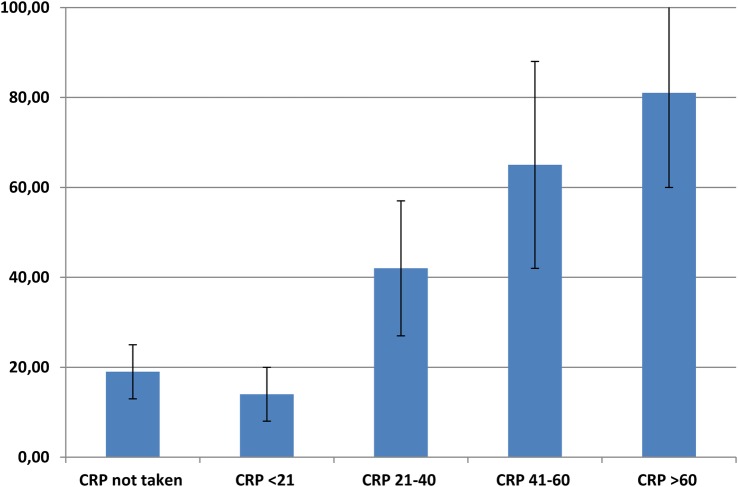
The total prescription rate of antibiotics was 23%, phenoxymethylpenicillin was used in 67% of the cases. Findings on ear examination (OR 4.62; 95% CI 2.35 to 9.10), parents' assessment that the child has a bacterial infection (OR 2.45; 95% CI 1.17 to 5.13) and a C reactive protein (CRP) value >20 mg/L (OR 3.57; 95% CI 1.43 to 8.83) were significantly associated with prescription of antibiotics. Vomiting in the past 24 hours was negatively associated with prescription (OR 0.26; 95% CI 0.13 to 0.53). The main predictors significantly associated with referral to hospital were respiratory rate (OR 1.07; 95% CI 1.03 to 1.12), oxygen saturation <95% (OR 3.39; 95% CI 1.02 to 11.23), signs on auscultation (OR 5.57; 95% CI 1.96 to 15.84) and the parents' assessment before the consultation that the child needs hospitalisation (OR 414; 95% CI 26 to 6624).
CRP values >20 mg/L, findings on ear examination, use of paracetamol and no vomiting in the past 24 hours were significantly associated with antibiotic prescription. Affected respiration was a predictor for referral to hospital. The parents' assessment was also significantly associated with the outcomes.
NCT02496559; Results.
儿童急性呼吸道感染和发热在初级保健中极为常见。区分病毒感染和细菌感染具有挑战性。挪威抗生素处方率相对较低,但由于抗菌药物耐药性不断增加,该比率仍被认为过高。本研究的目的是确定儿童抗生素处方或转诊至医院的预测因素。
一项随机对照研究的二次分析。
挪威初级保健中的4个非工作时间服务机构和1个儿科急诊诊所。
401名年龄在0至6岁、有呼吸道症状和/或发热且前往非工作时间服务机构就诊的儿童。
记录了2个主要结果变量:抗生素处方和转诊至医院。
抗生素总处方率为23%,67%的病例使用了青霉素V钾。耳部检查结果(比值比[OR]4.62;95%置信区间[CI]2.35至9.10)、家长认为孩子患有细菌感染(OR 2.45;95% CI 1.17至5.13)以及C反应蛋白(CRP)值>20mg/L(OR 3.57;95% CI 1.43至8.83)与抗生素处方显著相关。过去24小时内呕吐与处方呈负相关(OR 0.26;95% CI 0.13至0.53)。与转诊至医院显著相关的主要预测因素为呼吸频率(OR 1.07;95% CI 1.03至1.12)、血氧饱和度<95%(OR 3.39;95% CI 1.02至11.23)、听诊体征(OR 5.57;95% CI 1.96至15.84)以及家长在咨询前认为孩子需要住院治疗(OR 414;95% CI 26至6624)。
CRP值>20mg/L、耳部检查结果、使用对乙酰氨基酚以及过去24小时内未呕吐与抗生素处方显著相关。呼吸受影响是转诊至医院的一个预测因素。家长的评估也与结果显著相关。
NCT02496559;结果