Department of Community, Primary Care and Emergency Medicine, Division of Emergency Medicine.
Department of Interdisciplinary Centers and Medical Logistics, Division of Emergency Medicine, Centre Hospitalier Universitaire Vaudois, Lausanne, Switzerland.
Eur J Emerg Med. 2018 Aug;25(4):264-269. doi: 10.1097/MEJ.0000000000000449.
The Swiss Emergency Triage Scale (SETS) is a four-level emergency scale that previously showed moderate reliability and high rates of undertriage due to a lack of standardization. It was revised to better standardize the measurement and interpretation of vital signs during the triage process.
The aim of this study was to explore the inter-rater and test-retest reliability, and the rate of correct triage of the revised SETS.
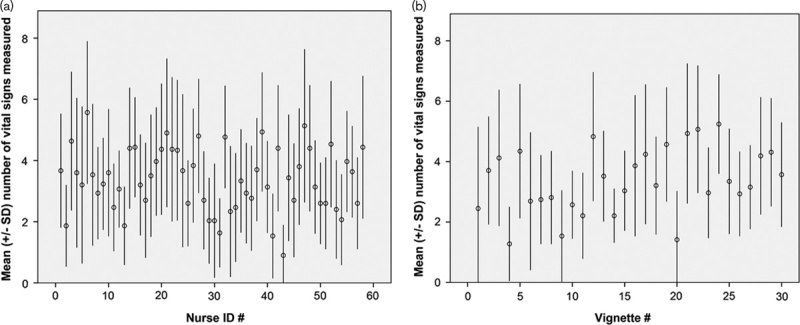
Thirty clinical scenarios were evaluated twice at a 3-month interval using an interactive computerized triage simulator by 58 triage nurses at an urban teaching emergency department admitting 60 000 patients a year. Inter-rater and test-retest reliabilities were determined using κ statistics. Triage decisions were compared with a gold standard attributed by an expert panel. Rates of correct triage, undertriage, and overtriage were computed. A logistic regression model was used to identify the predictors of correct triage.
A total of 3387 triage situations were analyzed. Inter-rater reliability showed substantial agreement [mean κ: 0.68; 95% confidence interval (CI): 0.60-0.78] and test-retest almost perfect agreement (mean κ: 0.86; 95% CI: 0.84-0.88). The rate of correct triage was 84.1%, and rates of undertriage and overtriage were 7.2 and 8.7%, respectively. Vital sign measurement was an independent predictor of correct triage (odds ratios for correct triage: 1.29 for each additional vital sign measured, 95% CI: 1.20-1.39).
The revised SETS incorporating standardized vital sign measurement and interpretation during the triage process resulted in high reliability and low rates of mistriage.
瑞士急救分类量表(SETS)是一个四级急救分类量表,由于缺乏标准化,其之前的可靠性为中等,且过度分类的比例较高。该量表经过修订,以更好地规范在分诊过程中对生命体征的测量和解读。
本研究旨在探讨修订版 SETS 的组内和重测信度,以及正确分诊的比例。
3 个月间隔内,58 名分诊护士使用城市教学急诊室的交互式计算机分诊模拟器评估了 30 个临床场景,该急诊室每年接诊 6 万例患者。使用 κ 统计量评估组内和重测信度。将分诊决策与专家小组确定的金标准进行比较。计算正确分诊、分诊不足和分诊过度的比例。使用逻辑回归模型确定正确分诊的预测因素。
共分析了 3387 次分诊情况。组内信度显示出高度一致性(平均 κ:0.68;95%置信区间 [CI]:0.60-0.78),重测信度几乎为完美一致(平均 κ:0.86;95% CI:0.84-0.88)。正确分诊的比例为 84.1%,分诊不足和过度分诊的比例分别为 7.2%和 8.7%。生命体征测量是正确分诊的独立预测因素(正确分诊的比值比:每增加一个测量的生命体征,95% CI:1.20-1.39)。
在分诊过程中纳入标准化的生命体征测量和解读的修订版 SETS 可实现高可靠性和低误诊率。