Haque Farhana, Ball Robyn L, Khatun Selina, Ahmed Mujaddeed, Kache Saraswati, Chisti Mohammod Jobayer, Sarker Shafiqul Alam, Maples Stace D, Pieri Dane, Vardhan Korrapati Teja, Sarnquist Clea, Federspiel Nancy, Rahman Muhammad Waliur, Andrews Jason R, Rahman Mahmudur, Nelson Eric Jorge
Institute of Epidemiology, Disease Control, and Research (IEDCR), Bangladesh Ministry of Health and Family Welfare, Dhaka, Bangladesh.
Infectious Diseases Division (IDD), International Centre for Diarrhoeal Disease Research, Bangladesh (icddr,b), Dhaka, Bangladesh.
PLoS Negl Trop Dis. 2017 Jan 19;11(1):e0005290. doi: 10.1371/journal.pntd.0005290. eCollection 2017 Jan.
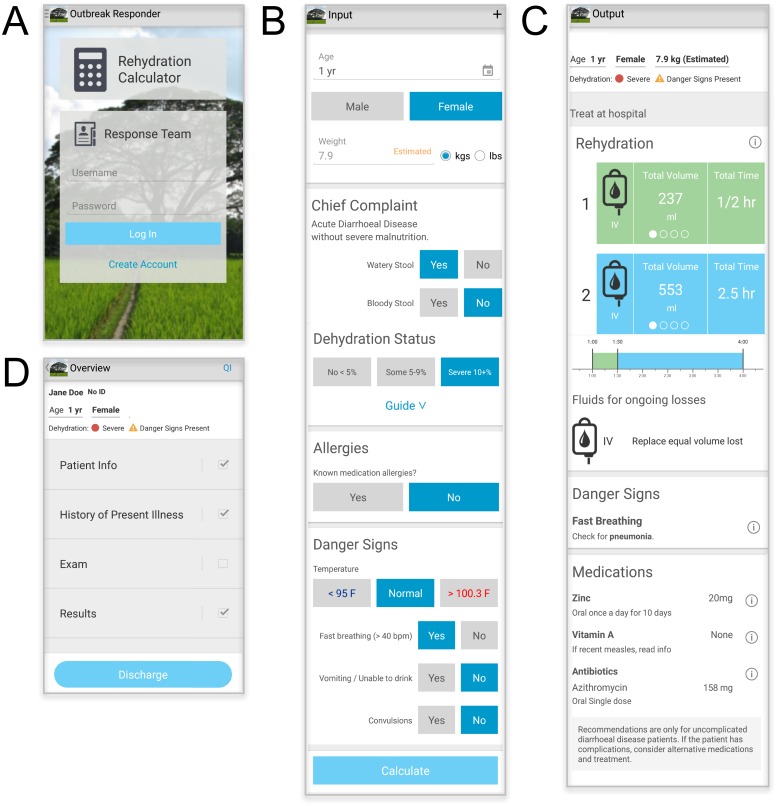
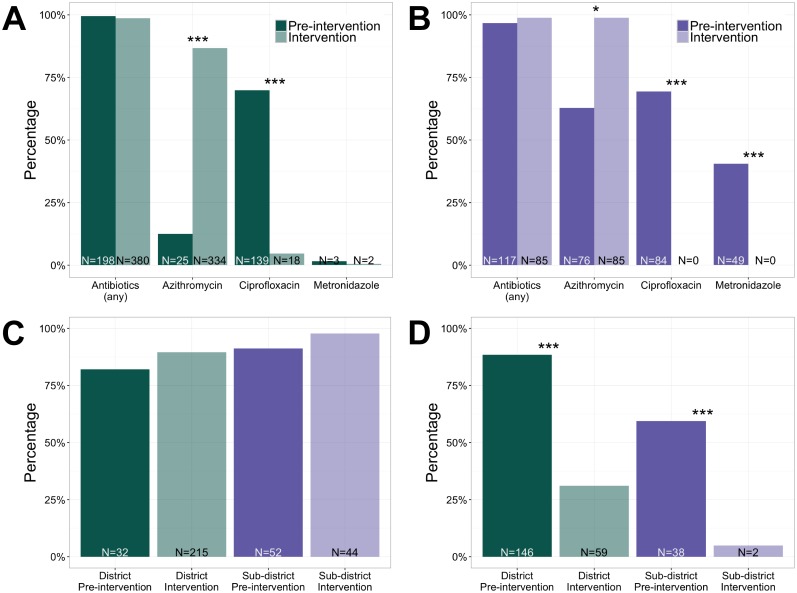
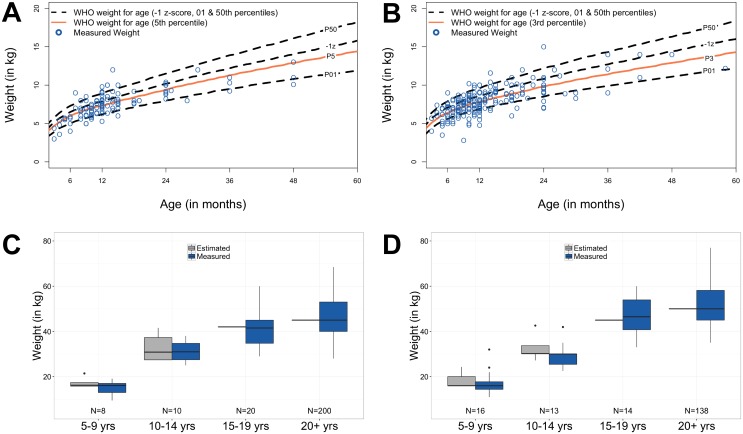
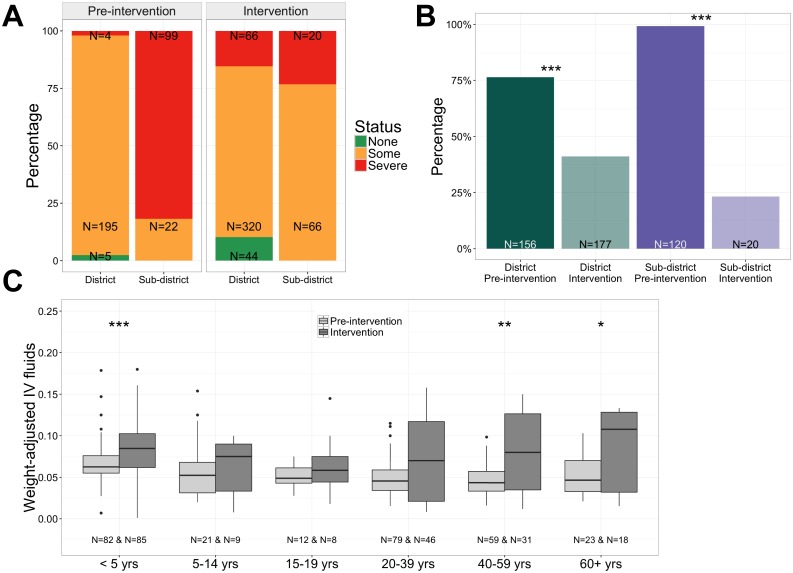
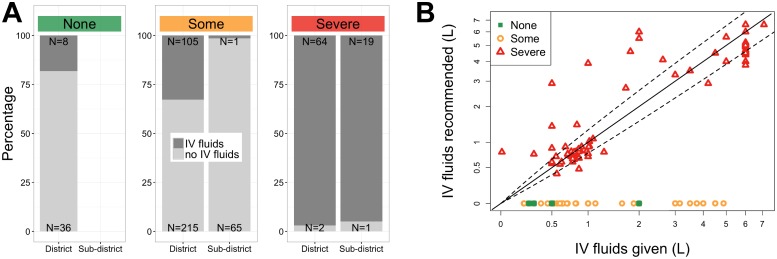
The emergence of mobile technology offers new opportunities to improve clinical guideline adherence in resource-limited settings. We conducted a clinical pilot study in rural Bangladesh to evaluate the impact of a smartphone adaptation of the World Health Organization (WHO) diarrheal disease management guidelines, including a modality for age-based weight estimation. Software development was guided by end-user input and evaluated in a resource-limited district and sub-district hospital during the fall 2015 cholera season; both hospitals lacked scales which necessitated weight estimation. The study consisted of a 6 week pre-intervention and 6 week intervention period with a 10-day post-discharge follow-up. Standard of care was maintained throughout the study with the exception that admitting clinicians used the tool during the intervention. Inclusion criteria were patients two months of age and older with uncomplicated diarrheal disease. The primary outcome was adherence to guidelines for prescriptions of intravenous (IV) fluids, antibiotics and zinc. A total of 841 patients were enrolled (325 pre-intervention; 516 intervention). During the intervention, the proportion of prescriptions for IV fluids decreased at the district and sub-district hospitals (both p < 0.001) with risk ratios (RRs) of 0.5 and 0.2, respectively. However, when IV fluids were prescribed, the volume better adhered to recommendations. The proportion of prescriptions for the recommended antibiotic azithromycin increased (p < 0.001 district; p = 0.035 sub-district) with RRs of 6.9 (district) and 1.6 (sub-district) while prescriptions for other antibiotics decreased; zinc adherence increased. Limitations included an absence of a concurrent control group and no independent dehydration assessment during the pre-intervention. Despite limitations, opportunities were identified to improve clinical care, including better assessment, weight estimation, and fluid/ antibiotic selection. These findings demonstrate that a smartphone-based tool can improve guideline adherence. This study should serve as a catalyst for a randomized controlled trial to expand on the findings and address limitations.
移动技术的出现为在资源有限的环境中提高临床指南的依从性提供了新的机会。我们在孟加拉国农村地区进行了一项临床试点研究,以评估对世界卫生组织(WHO)腹泻病管理指南进行智能手机适配的影响,其中包括一种基于年龄的体重估计方法。软件开发以最终用户的意见为指导,并在2015年秋季霍乱季节期间在资源有限的地区和分区医院进行了评估;两家医院都没有秤,因此需要进行体重估计。该研究包括为期6周的干预前阶段和为期6周的干预期,并在出院后进行了10天的随访。在整个研究过程中,除了干预期间接诊的临床医生使用该工具外,均维持了标准治疗。纳入标准为年龄在两个月及以上且患有非复杂性腹泻病的患者。主要结果是对静脉输液、抗生素和锌的处方遵循指南情况。总共招募了841名患者(干预前325名;干预组516名)。在干预期间,地区和分区医院静脉输液处方的比例均下降(均p<0.001),风险比(RR)分别为0.5和0.2。然而,当开具静脉输液处方时,输液量更符合推荐标准。推荐抗生素阿奇霉素的处方比例增加(地区p<0.001;分区p = 0.035),RR分别为6.9(地区)和1.6(分区),而其他抗生素的处方减少;锌的遵循情况增加。局限性包括缺乏同期对照组以及干预前没有独立的脱水评估。尽管存在局限性,但仍发现了改善临床护理的机会,包括更好的评估、体重估计以及液体/抗生素选择。这些发现表明,基于智能手机的工具可以提高指南的依从性。本研究应成为开展随机对照试验的催化剂,以扩展研究结果并解决局限性问题。