Department of Public Health and Primary Care, University of Cambridge, Cambridge, England2Medical Research Council Unit for Lifelong Health and Ageing at University College London, London, England.
Centre for Dementia Prevention, University of Edinburgh, Edinburgh, Scotland.
JAMA Psychiatry. 2017 Mar 1;74(3):244-251. doi: 10.1001/jamapsychiatry.2016.3423.
Delirium is associated with accelerated cognitive decline. The pathologic substrates of this association are not yet known, that is, whether they are the same as those associated with dementia, are independent, or are interrelated.
To examine whether the accelerated cognitive decline observed after delirium is independent of the pathologic processes of classic dementia.
DESIGN, SETTING, AND PARTICIPANTS: Harmonized data from 987 individual brain donors from 3 observational cohort studies with population-based sampling (Vantaa 85+, Cambridge City Over-75s Cohort, Cognitive Function and Ageing Study) performed from January 1, 1985, through December 31, 2011, with a median follow-up of 5.2 years until death, were used in this study. Neuropathologic assessments were performed with investigators masked to clinical data. Data analysis was performed from January 1, 2012, through December 31, 2013. Clinical characteristics of brain donors were not different from the rest of the cohort. Outcome ascertainment was complete given that the participants were brain donors.
Delirium (never vs ever) and pathologic burden of neurofibrillary tangles, amyloid plaques, vascular lesions, and Lewy bodies. Effects modeled using random-effects linear regression and interactions between delirium and pathologic burden were assessed.
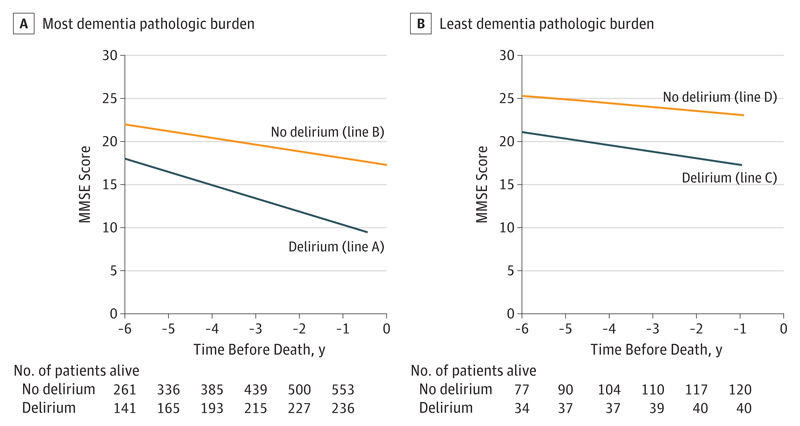
Change in Mini-Mental State Examination (MMSE) scores during the 6 years before death.
There were 987 participants (290 from Vantaa 85+, 241 from the Cambridge City Over-75s Cohort, and 456 from the Cognitive Function and Ageing Study) with neuropathologic data; mean (SD) age at death was 90 (6.4) years, including 682 women (69%). The mean MMSE score 6 years before death was 24.7 points. The 279 individuals with delirium (75% women) had worse initial scores (-2.8 points; 95% CI, -4.5 to -1.0; P < .001). Cognitive decline attributable to delirium was -0.37 MMSE points per year (95% CI, -0.60 to -0.13; P < .001). Decline attributable to the pathologic processes of dementia was -0.39 MMSE points per year (95% CI, -0.57 to -0.22; P < .001). However, the combination of delirium and the pathologic processes of dementia resulted in the greatest decline, in which the interaction contributed an additional -0.16 MMSE points per year (95% CI, -0.29 to -0.03; P = .01). The multiplicative nature of these variables resulted in individuals with delirium and the pathologic processes of dementia declining 0.72 MMSE points per year faster than age-, sex-, and educational level-matched controls.
Delirium in the presence of the pathologic processes of dementia is associated with accelerated cognitive decline beyond that expected for delirium or the pathologic process itself. These findings suggest that additional unmeasured pathologic processes specifically relate to delirium. Age-related cognitive decline has many contributors, and these findings at the population level support a role for delirium acting independently and multiplicatively to the pathologic processes of classic dementia.
谵妄与认知能力加速下降有关。但与这种关联相关的病理基础尚不清楚,即它们是否与痴呆相关的病理基础相同,是否独立,还是相互关联。
研究谵妄后观察到的认知能力加速下降是否与经典痴呆的病理过程无关。
设计、地点和参与者:本研究使用了来自 3 项基于人群抽样的观察队列研究(万塔 85+、剑桥市 75 岁以上人群队列、认知功能与衰老研究)的 987 名个体脑捐献者的协调数据。这些数据于 1985 年 1 月 1 日至 2011 年 12 月 31 日期间采集,中位随访时间为 5.2 年,直至死亡。进行神经病理学评估的研究人员对临床数据进行了盲法处理。数据分析于 2012 年 1 月 1 日至 2013 年 12 月 31 日进行。脑捐献者的临床特征与队列的其余部分没有差异。由于参与者是脑捐献者,因此可以完整地确定结果。
谵妄(无 vs 有)和神经原纤维缠结、淀粉样斑块、血管病变和路易体的病理负担。使用随机效应线性回归来模拟效果,并评估谵妄与病理负担之间的相互作用。
在死亡前的 6 年内,Mini-Mental State Examination(MMSE)评分的变化。
共有 987 名参与者(290 名来自万塔 85+,241 名来自剑桥市 75 岁以上人群队列,456 名来自认知功能与衰老研究)有神经病理学数据;死亡时的平均(SD)年龄为 90(6.4)岁,包括 682 名女性(69%)。死亡前 6 年的平均 MMSE 得分为 24.7 分。279 名患有谵妄(75%为女性)的患者初始得分更差(-2.8 分;95%CI,-4.5 至-1.0;P<0.001)。谵妄导致的认知下降为每年-0.37 MMSE 点(95%CI,-0.60 至-0.13;P<0.001)。痴呆病理过程导致的下降为每年-0.39 MMSE 点(95%CI,-0.57 至-0.22;P<0.001)。然而,谵妄和痴呆病理过程的结合导致了最大的下降,其中相互作用导致每年额外下降-0.16 MMSE 点(95%CI,-0.29 至-0.03;P=0.01)。这些变量的乘法性质导致患有谵妄和痴呆病理过程的个体每年比年龄、性别和教育水平匹配的对照组下降 0.72 MMSE 点更快。
在痴呆病理过程存在的情况下发生谵妄,与预期的谵妄或病理过程本身相比,认知能力下降加速。这些发现表明,有其他未测量的病理过程与谵妄特别相关。与年龄相关的认知衰退有许多原因,这些在人群水平上的发现支持谵妄独立且倍增地作用于经典痴呆的病理过程。