Sepulveda Esteban, Leonard Maeve, Franco Jose G, Adamis Dimitrios, McCarthy Geraldine, Dunne Colum, Trzepacz Paula T, Gaviria Ana M, de Pablo Joan, Vilella Elisabet, Meagher David J
Hospital Psiquiatric Universitari Institut Pere Mata, IISPV, Universitat Rovira i Virgili, Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Reus, Tarragona, Spain.
University of Limerick Graduate Entry Medical School, Limerick, Ireland; Cognitive Impairment Research Group, Centre for Interventions in Infection, Inflammation and Immunity (4i), Graduate Entry Medical School, University of Limerick, Ireland.
Alzheimers Dement (Amst). 2016 Dec 1;7:1-10. doi: 10.1016/j.dadm.2016.11.002. eCollection 2017.
Subsyndromal delirium (SSD) complicates diagnosis of delirium and dementia, although there is little research comparing their symptom profiles.
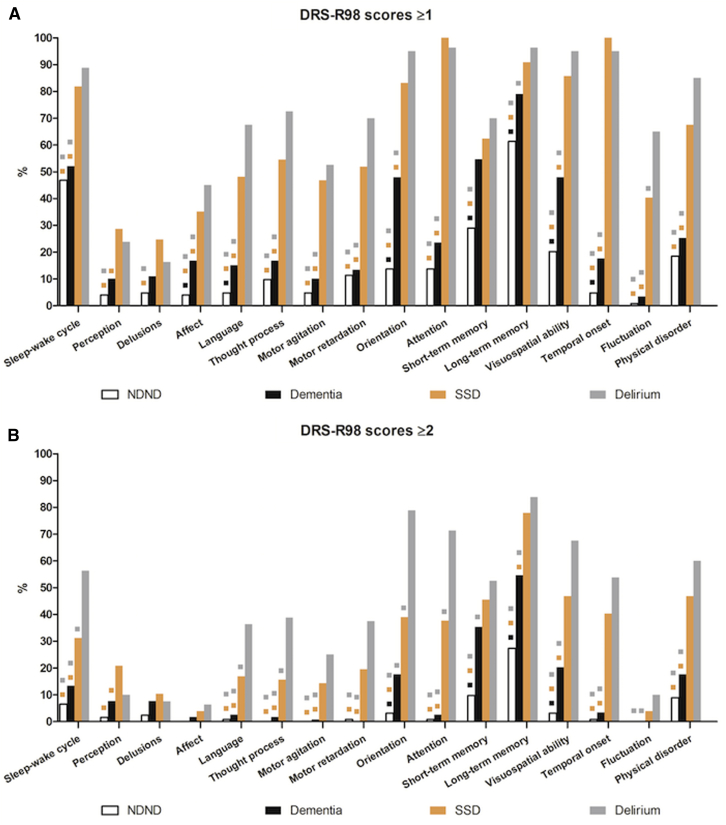
Cross-sectional study of 400 elderly patients' admission to a general hospital or nursing home diagnosed with delirium, SSD, dementia, or no-delirium/no-dementia (NDND). Symptom profiles were assessed using the Delirium Rating Scale-Revised-98 (DRS-R98).
Twenty percent patients had delirium, 19.3% had SSD, 29.8% had dementia-only, and 31% had NDND. Eighty-one percent of subsyndromal and 76% of delirium groups had comorbid dementia. DRS-R98 scores showed ascending severity from NDND < dementia-only < SSD < delirium. DRS-R98 scores for items evaluating the three core symptom domains (cognitive, higher-order thinking, and circadian) distinguished SSD from delirium and both from nondelirium groups. DRS-R98 profiles were essentially the same in delirium and SSD subgroups with or without dementia, although total scale scores were generally higher when in comorbid subgroups.
SSD shared characteristic core domain symptoms with delirium, which distinguished each from nondelirium groups, although severity was intermediate in the subsyndromal group. Delirium core symptoms overshadowed the dementia phenotype when comorbid. Milder disturbances of delirium core domain symptoms are highly suggestive of SSD.
尽管很少有研究比较亚综合征性谵妄(SSD)和痴呆症的症状特征,但SSD会使谵妄和痴呆症的诊断变得复杂。
对400名入住综合医院或疗养院的老年患者进行横断面研究,这些患者被诊断为谵妄、SSD、痴呆症或无谵妄/无痴呆症(NDND)。使用谵妄评定量表修订版98(DRS-R98)评估症状特征。
20%的患者患有谵妄,19.3%患有SSD,29.8%仅患有痴呆症,31%患有NDND。亚综合征组81%和谵妄组76%的患者患有共病性痴呆症。DRS-R98评分显示严重程度从NDND<仅痴呆症<SSD<谵妄呈上升趋势。评估三个核心症状领域(认知、高阶思维和昼夜节律)的项目的DRS-R98评分将SSD与谵妄区分开来,并将两者与非谵妄组区分开来。无论是否患有痴呆症,谵妄和SSD亚组的DRS-R98特征基本相同,尽管共病亚组的总分通常更高。
SSD与谵妄共享特征性核心领域症状,并将两者与非谵妄组区分开来,尽管亚综合征组的严重程度处于中间水平。当共病时,谵妄的核心症状掩盖了痴呆症的表型。谵妄核心领域症状的较轻紊乱高度提示SSD。