Croome Kristopher P, Lee David D, Harnois Denise, Taner C Burcin
Department of Transplant, Mayo Clinic Florida, Jacksonville, Florida.
PLoS One. 2017 Jan 25;12(1):e0170673. doi: 10.1371/journal.pone.0170673. eCollection 2017.
Several studies have investigated the effects following the implementation of the "Share 35" policy; however none have investigated what effect this policy change has had on waitlist and liver transplantation (LT) outcomes for hepatocellular carcinoma(HCC).
Data were obtained from the UNOS database and a comparison of the 2 years post-Share 35 with data from the 2 years pre-Share 35 was performed.
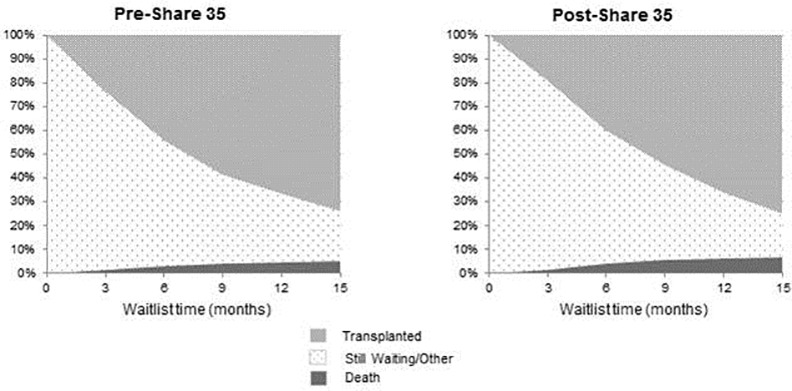
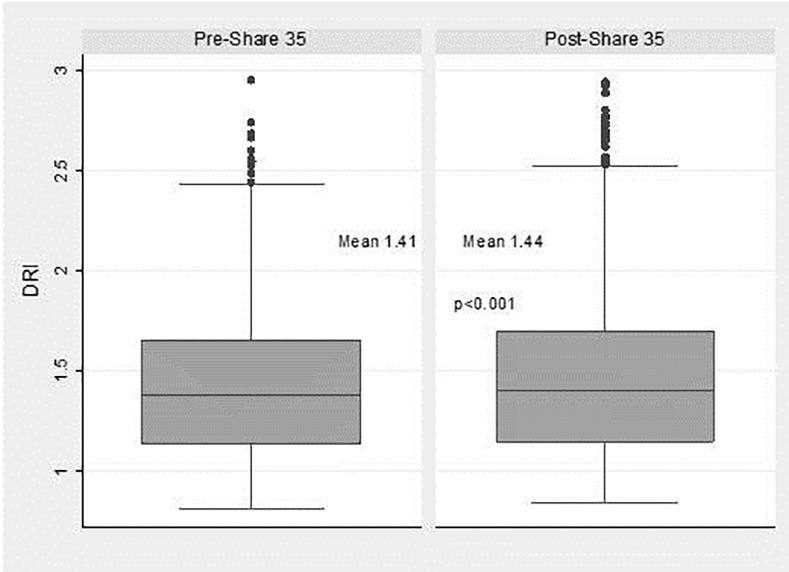
In the pre-Share35 era, 23% of LT were performed for HCC exceptions compared to 22% of LT in the post-Share35 era (p = 0.21). No difference in wait-time for HCC patients was seen in any of the UNOS regions between the 2 eras. Competing risk analysis demonstrated that HCC candidates in post-Share 35 era were more likely to die or be delisted for "too sick" while waiting (7.2% vs. 5.3%; p = 0.005) within 15 months. A higher proportion of ECD (p<0.001) and DCD (p<0.001) livers were used for patients transplanted for HCC, while lower DRI organs were used for those patients transplanted with a MELD≥35 between the 2 eras (p = 0.007).
No significant change to wait-time for patients listed for HCC was seen following implementation of "Share 35". Transplant program behavior has changed resulting use of higher proportion of ECD and DCD liver grafts for patients with HCC. A higher rate of wait list mortality was observed in patients with HCC in the post-Share 35 era.
多项研究调查了“共享35分”政策实施后的影响;然而,尚无研究调查这一政策变化对肝细胞癌(HCC)等待名单和肝移植(LT)结果产生了何种影响。
数据取自器官共享联合网络(UNOS)数据库,并将“共享35分”政策实施后的两年数据与该政策实施前两年的数据进行了比较。
在“共享35分”政策实施前的时代,23%的肝移植是针对肝癌例外情况进行的,而在“共享35分”政策实施后的时代,这一比例为22%(p = 0.21)。在两个时代之间,UNOS的任何地区,肝癌患者的等待时间均无差异。竞争风险分析表明,在“共享35分”政策实施后的时代,肝癌候选患者在等待期间(15个月内)更有可能因“病情过重”而死亡或被从等待名单中除名(7.2%对5.3%;p = 0.005)。在两个时代之间,更高比例的边缘供肝(ECD)(p<0.001)和心死亡后供肝(DCD)(p<0.001)被用于肝癌移植患者,而较低供肝风险指数(DRI)的器官则被用于终末期肝病模型(MELD)评分≥35分的移植患者(p = 0.007)。
“共享35分”政策实施后,肝癌等待患者的等待时间没有显著变化。移植项目行为发生了改变,导致更高比例的ECD和DCD肝移植用于肝癌患者。在“共享35分”政策实施后的时代,肝癌患者等待名单上的死亡率更高。