Yamauchi Yoshikane, Isaka Mitsuhiro, Ando Kamon, Mori Keita, Kojima Hideaki, Maniwa Tomohiro, Takahashi Shoji, Ando Eiji, Ohde Yasuhisa
Division of General Thoracic Surgery, Shizuoka Cancer Center, 1007 Shimonagakubo, Nagaizumi, Shizuoka, 411-8777, Japan.
Division of Anesthesiology, Shizuoka Cancer Center, Shizuoka, Japan.
J Cardiothorac Surg. 2017 Jan 25;12(1):5. doi: 10.1186/s13019-017-0566-8.
Thoracic epidural analgesia (EDA) is the gold standard for pain control after thoracotomy. However, because of its severe side effects, it is contraindicated in patients taking anticoagulant or antiplatelet drugs. In addition, some patients' anatomy can make epidural catheter insertion challenging. We therefore investigated the safety and efficacy of paravertebral block (PVB) using a thoracoscopic insertion technique, which avoids damage to the parietal pleura, for postoperative pain after thoracotomy.
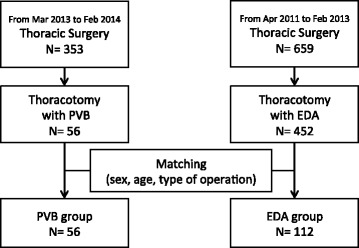
Patients who underwent thoracotomy with thoracic PVB in our hospital between March 2013 and March 2014 were examined retrospectively. Prior to creating the thoracotomy incision, a catheter for PVB was inserted percutaneously into the paravertebral space under thoracoscopic guidance. A matched-pair control group was selected at a 1:2 ratio from patients who underwent thoracotomy with thoracic EDA in our hospital from April 2011 to February 2013. Pain control and side effects were compared between groups and the results statistically analyzed.
Thoracic PVB was performed in 56 patients during this period, and 112 patients were selected as matched controls. Numeric Rating Scale scores on postoperative day 2 did not differ significantly between the PVB group (3.25 ± 1.80) and the EDA group (3.56 ± 2.05) (p = 0.334). In terms of side effects, urinary retention occurred less frequently in thoracic PVB patients (p = 0.03).
Under the conditions of the present study, continuous thoracic PVB was at least as effective as epidural analgesia for postoperative pain control after thoracotomy with lung resection.
胸段硬膜外镇痛(EDA)是开胸术后疼痛控制的金标准。然而,由于其严重的副作用,在服用抗凝或抗血小板药物的患者中为禁忌。此外,一些患者的解剖结构可能使硬膜外导管插入具有挑战性。因此,我们研究了采用胸腔镜插入技术的椎旁阻滞(PVB)用于开胸术后疼痛的安全性和有效性,该技术可避免损伤壁层胸膜。
回顾性研究2013年3月至2014年3月在我院接受开胸手术并行胸段PVB的患者。在开胸切口形成前,在胸腔镜引导下经皮将PVB导管插入椎旁间隙。从2011年4月至2013年2月在我院接受开胸手术并行胸段EDA的患者中按1:2比例选取配对对照组。比较两组间的疼痛控制情况和副作用,并对结果进行统计学分析。
在此期间56例患者接受了胸段PVB,112例患者被选为配对对照。PVB组术后第2天数字评分量表得分(3.25±1.80)与EDA组(3.56±2.05)相比无显著差异(p = 0.334)。在副作用方面,胸段PVB患者尿潴留发生率较低(p = 0.03)。
在本研究条件下,持续胸段PVB在肺切除开胸术后疼痛控制方面至少与硬膜外镇痛效果相当。