Valikodath Nita G, Newman-Casey Paula Anne, Lee Paul P, Musch David C, Niziol Leslie M, Woodward Maria A
Department of Ophthalmology and Visual Sciences, University of Michigan Medical School, Ann Arbor2currently a medical student at the University of Michigan Medical School, Ann Arbor.
Department of Ophthalmology and Visual Sciences, University of Michigan Medical School, Ann Arbor3Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor.
JAMA Ophthalmol. 2017 Mar 1;135(3):225-231. doi: 10.1001/jamaophthalmol.2016.5551.
Accurate documentation of patient symptoms in the electronic medical record (EMR) is important for high-quality patient care.
To explore inconsistencies between patient self-report on an Eye Symptom Questionnaire (ESQ) and documentation in the EMR.
DESIGN, SETTING, AND PARTICIPANTS: This investigation was an observational study in comprehensive ophthalmology and cornea clinics at an academic institution among a convenience sample of 192 consecutive eligible patients, of whom 30 declined participation. Patients were recruited at the Kellogg Eye Center from October 1, 2015, to January 31, 2016. Patients were eligible to be included in the study if they were 18 years or older.
Concordance of symptoms reported on an ESQ with data recorded in the EMR. Agreement of symptom report was analyzed using κ statistics and McNemar tests. Disagreement was defined as a negative symptom report or no mention of a symptom in the EMR for patients who reported moderate to severe symptoms on the ESQ. Logistic regression was used to investigate if patient factors, physician characteristics, or diagnoses were associated with the probability of disagreement for symptoms of blurry vision, pain or discomfort, and redness.
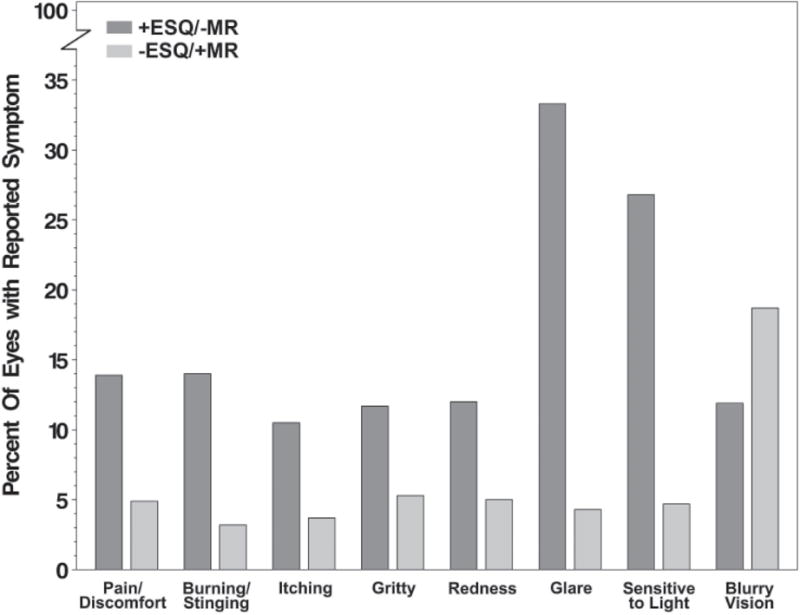
A total of 162 patients (324 eyes) were included. The mean (SD) age of participants was 56.6 (19.4) years, 62.3% (101 of 162) were female, and 84.9% (135 of 159) were white. At the participant level, 33.8% (54 of 160) had discordant reporting of blurry vision between the ESQ and EMR. Likewise, documentation was discordant for reporting glare (48.1% [78 of 162]), pain or discomfort (26.5% [43 of 162]), and redness (24.7% [40 of 162]), with poor to fair agreement (κ range, -0.02 to 0.42). Discordance of symptom reporting was more frequently characterized by positive reporting on the ESQ and lack of documentation in the EMR (Holm-adjusted McNemar P < .03 for 7 of 8 symptoms except for blurry vision [P = .59]). Return visits at which the patient reported blurry vision on the ESQ had increased odds of not reporting the symptom in the EMR compared with new visits (odds ratio, 5.25; 95% CI, 1.69-16.30; Holm-adjusted P = .045).
Symptom reporting was inconsistent between patient self-report on an ESQ and documentation in the EMR, with symptoms more frequently recorded on a questionnaire. These results suggest that documentation of symptoms based on EMR data may not provide a comprehensive resource for clinical practice or "big data" research.
在电子病历(EMR)中准确记录患者症状对于高质量的患者护理至关重要。
探讨患者在眼部症状问卷(ESQ)上的自我报告与EMR记录之间的不一致性。
设计、设置和参与者:本调查是一项在一所学术机构的综合眼科和角膜诊所进行的观察性研究,对192名连续符合条件的患者进行便利抽样,其中30人拒绝参与。2015年10月1日至2016年1月31日期间在凯洛格眼科中心招募患者。年龄在18岁及以上的患者有资格纳入本研究。
ESQ上报告的症状与EMR中记录的数据的一致性。使用κ统计量和McNemar检验分析症状报告的一致性。不一致被定义为对于在ESQ上报告中度至重度症状的患者,EMR中症状报告为阴性或未提及该症状。使用逻辑回归研究患者因素、医生特征或诊断是否与视力模糊、疼痛或不适以及眼红症状不一致的可能性相关。
共纳入162名患者(324只眼)。参与者的平均(标准差)年龄为56.6(19.4)岁,62.3%(162人中的101人)为女性,84.9%(159人中的135人)为白人。在参与者层面,33.8%(160人中的54人)在ESQ和EMR之间关于视力模糊的报告不一致。同样,在眩光(48.1%[162人中的78人])、疼痛或不适(26.5%[162人中的43人])和眼红(24.7%[162人中的40人])的报告方面,记录也不一致,一致性较差至一般(κ范围为 -0.02至0.42)。症状报告的不一致更常见的表现是ESQ上报告为阳性而EMR中未记录(除视力模糊外的8种症状中有7种经Holm校正的McNemar P <.03[视力模糊P = 0.59])。与初次就诊相比,患者在ESQ上报告视力模糊的复诊在EMR中未报告该症状的几率增加(优势比,5.25;95%可信区间,1.69 - 16.30;经Holm校正P = 0.045)。
患者在ESQ上的自我报告与EMR记录之间的症状报告不一致,症状更常记录在问卷上。这些结果表明,基于EMR数据的症状记录可能无法为临床实践或“大数据”研究提供全面的资源。