Oguejiofor Patrick, Chow Robert, Yim Kenneth, Jaar Bernard G
Department of Internal Medicine, University of Maryland School of Medicine, Baltimore, MD, USA.
Division of Nephrology, University of Maryland Medical Center Midtown Campus, Baltimore, MD, USA.
Case Rep Nephrol. 2017;2017:8596169. doi: 10.1155/2017/8596169. Epub 2017 Jan 3.
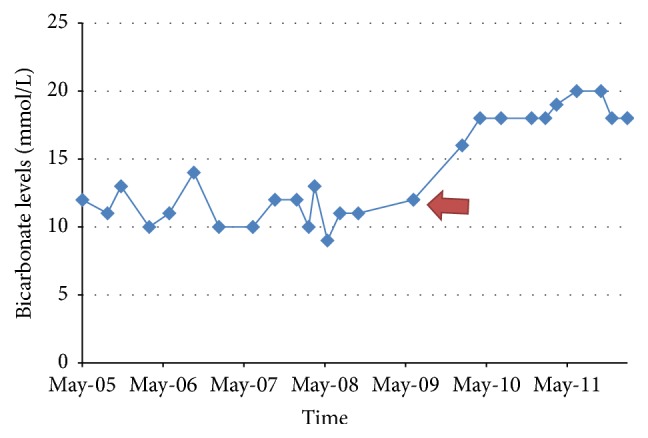
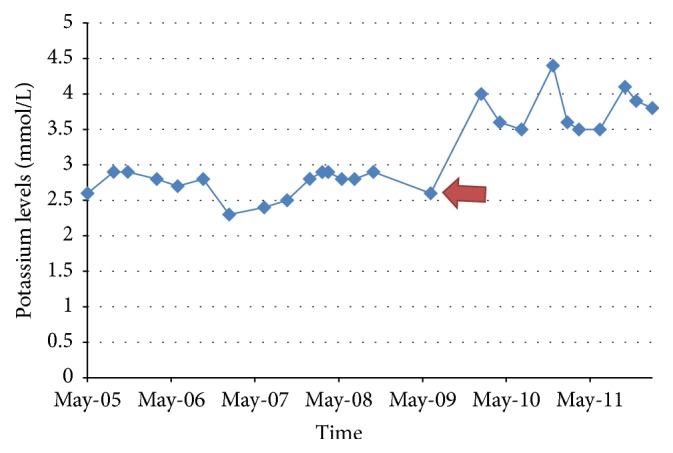
A 28-year-old female with history of hypothyroidism, Sjögren's Syndrome, and Systemic Lupus Erythematosus (SLE) presented with complaints of severe generalized weakness, muscle pain, nausea, vomiting, and anorexia. Physical examination was unremarkable. Laboratory test showed hypokalemia at 1.6 mmol/l, nonanion metabolic acidosis with HCO of 11 mmol/l, random urine pH of 7.0, and urine anion gap of 8 mmol/l. CT scan of the abdomen revealed bilateral nephrocalcinosis. A diagnosis of type 1 RTA likely secondary to Sjögren's Syndrome was made. She was started on citric acid potassium citrate with escalating dosages to a maximum dose of 60 mEq daily and potassium chloride over 5 years without significant improvement in serum K and HCO levels. She had multiple emergency room visits for persistent muscle pain, generalized weakness, and cardiac arrhythmias. Citric acid potassium citrate was then replaced with sodium bicarbonate at 15.5 mEq every 6 hours which was continued for 2 years without significant improvement in her symptoms and electrolytes. Amiloride 5 mg daily was added to her regimen as a potassium sparing treatment with dramatic improvement in her symptoms and electrolyte levels (as shown in the figures). Amiloride was increased to 10 mg daily and potassium supplementation was discontinued without affecting her electrolytes. Her sodium bicarbonate was weaned to 7.7 mEq daily.
一名28岁女性,有甲状腺功能减退、干燥综合征和系统性红斑狼疮(SLE)病史,出现严重全身乏力、肌肉疼痛、恶心、呕吐和厌食等症状。体格检查无异常。实验室检查显示低钾血症,血钾为1.6 mmol/L,非阴离子代谢性酸中毒,碳酸氢根为11 mmol/L,随机尿pH值为7.0,尿阴离子间隙为8 mmol/L。腹部CT扫描显示双侧肾钙质沉着症。诊断为1型肾小管酸中毒,可能继发于干燥综合征。开始给予枸橼酸钾,剂量逐渐增加至最大剂量每日60 mEq,并给予氯化钾,持续5年,但血清钾和碳酸氢根水平无明显改善。她因持续肌肉疼痛、全身乏力和心律失常多次前往急诊室就诊。随后将枸橼酸钾替换为每6小时15.5 mEq的碳酸氢钠,持续2年,其症状和电解质情况无明显改善。每日添加5 mg氨氯吡咪作为保钾治疗,其症状和电解质水平有显著改善(如图所示)。氨氯吡咪增至每日10 mg,停止补充钾,未影响其电解质情况。她的碳酸氢钠逐渐减至每日7.7 mEq。