Hall H Irene, Song Ruiguang, Tang Tian, An Qian, Prejean Joseph, Dietz Patricia, Hernandez Angela L, Green Timothy, Harris Norma, McCray Eugene, Mermin Jonathan
Centers for Disease Control and Prevention, Atlanta, GA, United States.
ICF, Atlanta, GA, United States.
JMIR Public Health Surveill. 2017 Feb 3;3(1):e8. doi: 10.2196/publichealth.7051.
The best indicator of the impact of human immunodeficiency virus (HIV) prevention programs is the incidence of infection; however, HIV is a chronic infection and HIV diagnoses may include infections that occurred years before diagnosis. Alternative methods to estimate incidence use diagnoses, stage of disease, and laboratory assays of infection recency. Using a consistent, accurate method would allow for timely interpretation of HIV trends.
The objective of our study was to assess the recent progress toward reducing HIV infections in the United States overall and among selected population segments with available incidence estimation methods.
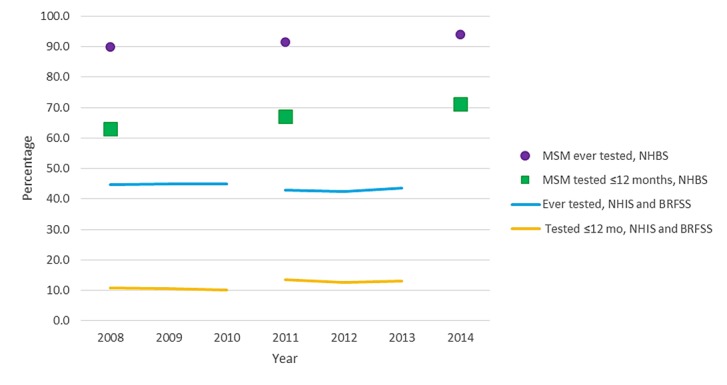
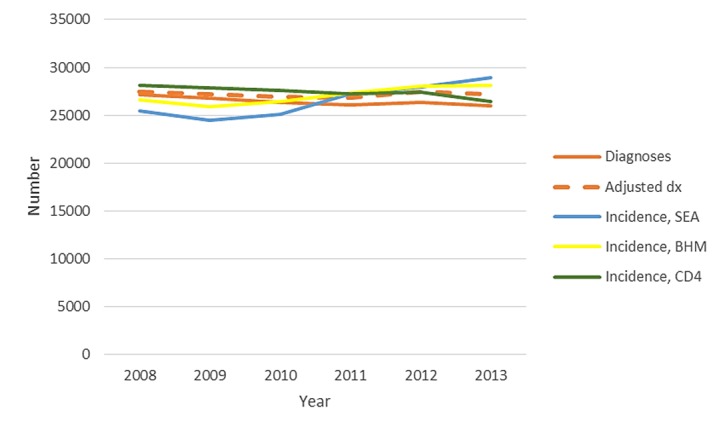
Data on cases of HIV infection reported to national surveillance for 2008-2013 were used to compare trends in HIV diagnoses, unadjusted and adjusted for reporting delay, and model-based incidence for the US population aged ≥13 years. Incidence was estimated using a biomarker for recency of infection (stratified extrapolation approach) and 2 back-calculation models (CD4 and Bayesian hierarchical models). HIV testing trends were determined from behavioral surveys for persons aged ≥18 years. Analyses were stratified by sex, race or ethnicity (black, Hispanic or Latino, and white), and transmission category (men who have sex with men, MSM).
On average, HIV diagnoses decreased 4.0% per year from 48,309 in 2008 to 39,270 in 2013 (P<.001). Adjusting for reporting delays, diagnoses decreased 3.1% per year (P<.001). The CD4 model estimated an annual decrease in incidence of 4.6% (P<.001) and the Bayesian hierarchical model 2.6% (P<.001); the stratified extrapolation approach estimated a stable incidence. During these years, overall, the percentage of persons who ever had received an HIV test or had had a test within the past year remained stable; among MSM testing increased. For women, all 3 incidence models corroborated the decreasing trend in HIV diagnoses, and HIV diagnoses and 2 incidence models indicated decreases among blacks and whites. The CD4 and Bayesian hierarchical models, but not the stratified extrapolation approach, indicated decreases in incidence among MSM.
HIV diagnoses and CD4 and Bayesian hierarchical model estimates indicated decreases in HIV incidence overall, among both sexes and all race or ethnicity groups. Further progress depends on effectively reducing HIV incidence among MSM, among whom the majority of new infections occur.
人类免疫缺陷病毒(HIV)预防项目影响的最佳指标是感染发生率;然而,HIV是一种慢性感染,HIV诊断可能包括诊断前数年发生的感染。估计发病率的替代方法使用诊断、疾病阶段和感染近期性的实验室检测。使用一致、准确的方法将有助于及时解读HIV趋势。
我们研究的目的是使用现有的发病率估计方法,评估美国总体及特定人群在减少HIV感染方面的近期进展。
利用2008 - 2013年向国家监测机构报告的HIV感染病例数据,比较HIV诊断的趋势,包括未调整及针对报告延迟进行调整后的趋势,以及≥13岁美国人群基于模型的发病率。使用感染近期性生物标志物(分层外推法)和2种反向计算模型(CD4和贝叶斯分层模型)估计发病率。通过对≥18岁人群的行为调查确定HIV检测趋势。分析按性别、种族或族裔(黑人、西班牙裔或拉丁裔、白人)以及传播类别(男男性行为者,MSM)进行分层。
平均而言,HIV诊断数从2008年的48,309例下降至2013年的39,270例,每年下降4.0%(P <.001)。针对报告延迟进行调整后,诊断数每年下降3.1%(P <.001)。CD4模型估计发病率每年下降4.6%(P <.001),贝叶斯分层模型估计为2.6%(P <.001);分层外推法估计发病率稳定。在这些年里,总体而言,曾经接受过HIV检测或在过去一年接受过检测的人群比例保持稳定;在MSM中检测率有所上升。对于女性,所有3种发病率模型都证实了HIV诊断数的下降趋势,HIV诊断数以及2种发病率模型表明黑人和白人中的发病率下降。CD4和贝叶斯分层模型表明MSM中的发病率下降,但分层外推法未显示此趋势。
HIV诊断数以及CD4和贝叶斯分层模型估计表明,总体上、男女及所有种族或族裔群体中的HIV发病率均有所下降。进一步的进展取决于有效降低MSM中的HIV发病率,新感染病例大多发生在该群体中。