Moore Frederick A, Phillips Stuart M, McClain Craig J, Patel Jayshil J, Martindale Robert G
1 University of Florida, Gainesville, Florida.
2 McMasters University, Hamilton, Canada.
Nutr Clin Pract. 2017 Apr;32(1_suppl):121S-127S. doi: 10.1177/0884533616687502. Epub 2017 Feb 6.
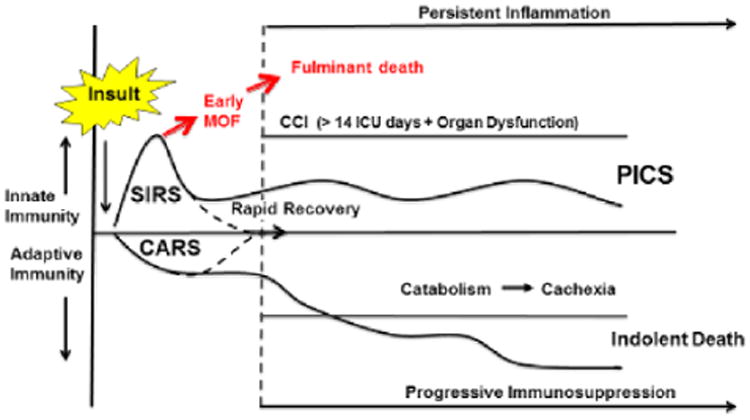
Despite tremendous advances in critical care, multiple-organ failure continues to be a significant problem. However, in recent years, far fewer patients with multiple-organ failure die early, but many experience ongoing immune dysregulation and are developing persistent inflammation, immunosuppression, and catabolism syndrome (PICS). Most PICS patients are discharged to nonhome destinations, fail to rehabilitate, and succumb to indolent death. From a nutrition perspective, patients with PICS experience persistent inflammation-induced cachexia despite evidenced-based recommended intensive care unit nutrition support. Recent basic and translational research indicates that prolonged expansion of myeloid-derived suppressor cells plays a central role in the pathogenesis of PICS. Myeloid-derived suppressor cells express arginase 1, which depletes arginine, causing immunosuppression and impaired wound healing. This is the rationale for arginine supplementation in PICS. Other nutrition support recommendations for PICS are based on inferences made from other patient populations who experience similar persistent inflammation-induced cachexia. These include patients with established cancers, major burns, and sarcopenia. These patients experience anabolic resistance, but studies show that this can be overcome by providing higher levels of protein and certain specific amino acids. Nutrition support guidelines recommend provision of >1.5 g/kg/d of protein and indicate that higher levels may be needed. Protein composition is also important. There is good evidence that leucine can promote anabolism in patients with cancer and sarcopenia. Finally, anabolic interventions-including intensive insulin, oxandrolone, propranolol, and resistance exercise-have proven to be effective in patients with major burns and are likely relevant in combating PICS cachexia.
尽管重症监护取得了巨大进展,但多器官功能衰竭仍然是一个重大问题。然而,近年来,多器官功能衰竭患者早期死亡的人数大幅减少,但许多患者仍存在持续的免疫失调,并正在发展为持续性炎症、免疫抑制和分解代谢综合征(PICS)。大多数PICS患者出院后前往非家庭场所,康复失败,并最终缓慢死亡。从营养角度来看,尽管有循证推荐的重症监护病房营养支持,但PICS患者仍会出现持续性炎症诱导的恶病质。最近的基础研究和转化研究表明,髓源性抑制细胞的长期扩增在PICS的发病机制中起核心作用。髓源性抑制细胞表达精氨酸酶1,该酶会消耗精氨酸,导致免疫抑制和伤口愈合受损。这就是在PICS中补充精氨酸的理论依据。PICS的其他营养支持建议是基于对其他经历类似持续性炎症诱导恶病质的患者群体的推断。这些患者包括确诊的癌症患者、大面积烧伤患者和肌肉减少症患者。这些患者存在合成代谢抵抗,但研究表明,通过提供更高水平的蛋白质和某些特定氨基酸可以克服这一问题。营养支持指南建议提供>1.5 g/kg/d的蛋白质,并指出可能需要更高的水平。蛋白质组成也很重要。有充分证据表明,亮氨酸可以促进癌症患者和肌肉减少症患者的合成代谢。最后,合成代谢干预措施——包括强化胰岛素、氧雄龙、普萘洛尔和抗阻运动——已被证明对大面积烧伤患者有效,并且可能与对抗PICS恶病质相关。