van der Zee Esther N, Egal Mohamud, Gommers Diederik, Groeneveld A B Johan
Department of Intensive Care, Erasmus MC, University Medical Center Rotterdam, Rotterdam, The Netherlands.
Erasmus MC, Room H-602, P.O. Box 2040, 3000 CA, Rotterdam, The Netherlands.
BMC Anesthesiol. 2017 Feb 10;17(1):22. doi: 10.1186/s12871-017-0316-4.
Oliguria is associated with a decreased kidney- and organ perfusion, leading to organ damage and increased mortality. While the effects of correcting oliguria on renal outcome have been investigated frequently, whether urine output is a modifiable risk factor for mortality or simply an epiphenomenon remains unclear. We investigated whether targeting urine output, defined as achieving and maintaining urine output above a predefined threshold, in hemodynamic management protocols affects 30-day mortality in perioperative and critical care.
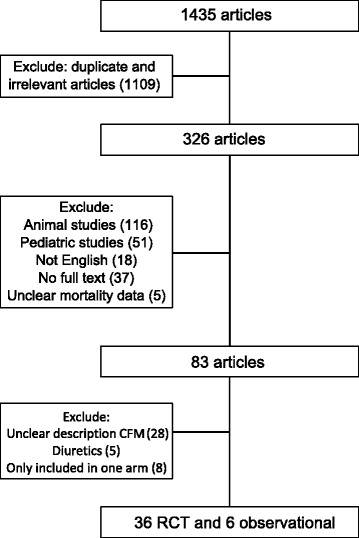
We performed a systematic review with a random-effects meta-analyses and meta-regression based on search strategy through MEDLINE, EMBASE and references in relevant articles. We included studies comparing conventional fluid management with goal-directed therapy and reporting whether urine output was used as target or not, and reporting 30-day mortality data in perioperative and critical care.
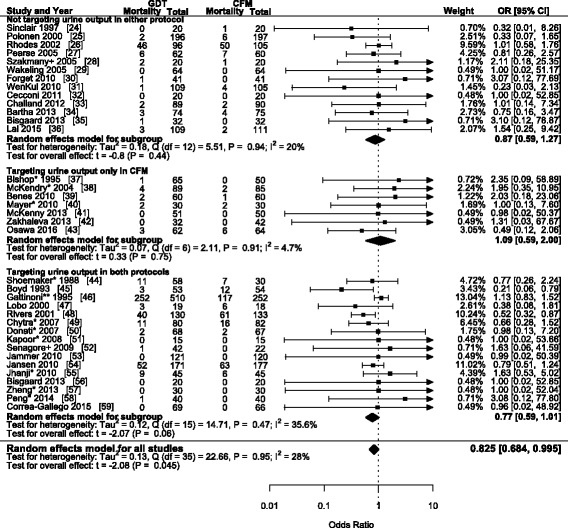
We found 36 studies in which goal-directed therapy reduced 30-day mortality (OR 0.825; 95% CI 0.684-0.995; P = 0.045). Targeting urine output within goal-directed therapy increased 30-day mortality (OR 2.66; 95% CI 1.06-6.67; P = 0.037), but not in conventional fluid management (OR 1.77; 95% CI 0.59-5.34; P = 0.305). After adjusting for operative setting, hemodynamic monitoring device, underlying etiology, use of vasoactive medication and year of publication, we found insufficient evidence to associate targeting urine output with a change in 30-day mortality (goal-directed therapy: OR 1.17; 95% CI 0.54-2.56; P = 0.685; conventional fluid management: OR 0.74; 95% CI 0.39-1.38; P = 0.334).
The principal finding of this meta-analysis is that after adjusting for confounders, there is insufficient evidence to associate targeting urine output with an effect on 30-day mortality. The paucity of direct data illustrates the need for further research on whether permissive oliguria should be a key component of fluid management protocols.
少尿与肾脏及器官灌注减少相关,可导致器官损害并增加死亡率。虽然纠正少尿对肾脏结局的影响已被频繁研究,但尿量是死亡率的一个可改变的危险因素还是仅仅是一种附带现象仍不明确。我们调查了在血流动力学管理方案中,将尿量目标设定为达到并维持在预定义阈值以上,是否会影响围手术期和重症监护中的30天死亡率。
我们基于通过MEDLINE、EMBASE及相关文章参考文献的检索策略,进行了一项随机效应荟萃分析和荟萃回归的系统评价。我们纳入了比较传统液体管理与目标导向治疗,并报告是否将尿量用作目标以及围手术期和重症监护中30天死亡率数据的研究。
我们发现36项研究中目标导向治疗降低了30天死亡率(比值比0.825;95%置信区间0.684 - 0.995;P = 0.045)。在目标导向治疗中设定尿量目标增加了30天死亡率(比值比2.66;95%置信区间1.06 - 6.67;P = 0.037),但在传统液体管理中并非如此(比值比1.77;95%置信区间0.59 - 5.34;P = 0.305)。在对手术环境、血流动力学监测设备、潜在病因、血管活性药物的使用及发表年份进行调整后,我们发现没有足够证据表明设定尿量目标与30天死亡率的变化相关(目标导向治疗:比值比1.17;95%置信区间0.54 - 2.56;P = 0.685;传统液体管理:比值比0.74;95%置信区间0.39 - 1.38;P = 0.334)。
这项荟萃分析的主要发现是,在对混杂因素进行调整后,没有足够证据表明设定尿量目标与对30天死亡率的影响相关。直接数据的匮乏表明需要进一步研究允许性少尿是否应成为液体管理方案的关键组成部分。