Glynne-Jones Robert, Sebag-Montefiore David, Meadows Helen M, Cunningham David, Begum Rubina, Adab Fawzi, Benstead Kim, Harte Robert J, Stewart Jill, Beare Sandy, Hackshaw Allan, Kadalayil Latha
Mount Vernon Centre for Cancer Treatment, Northwood, Leeds, UK.
University of Leeds, Leeds Cancer Centre, Leeds, UK.
Lancet Oncol. 2017 Mar;18(3):347-356. doi: 10.1016/S1470-2045(17)30071-2. Epub 2017 Feb 11.
Guidelines for anal cancer recommend assessment of response at 6-12 weeks after starting treatment. Using data from the ACT II trial, we determined the optimum timepoint to assess clinical tumour response after chemoradiotherapy.
The previously reported ACT II trial was a phase 3 randomised trial of patients of any age with newly diagnosed, histologically confirmed, squamous cell carcinoma of the anus without metastatic disease from 59 centres in the UK. We randomly assigned patients (by minimisation) to receive either intravenous mitomycin (one dose of 12 mg/m on day 1) or intravenous cisplatin (one dose of 60 mg/m on days 1 and 29), with intravenous fluorouracil (one dose of 1000 mg/m per day on days 1-4 and 29-32) and radiotherapy (50·4 Gy in 28 daily fractions); and also did a second randomisation after initial therapy to maintenance chemotherapy (fluorouracil and cisplatin) or no maintenance chemotherapy. The primary outcome was complete clinical response (the absence of primary and nodal tumour by clinical examination), in addition to overall survival and progression-free survival from time of randomisation. In this post-hoc analysis, we analysed complete clinical response at three timepoints: 11 weeks from the start of chemoradiotherapy (assessment 1), 18 weeks from the start of chemoradiotherapy (assessment 2), and 26 weeks from the start of chemoradiotherapy (assessment 3) as well as the overall and progression-free survival estimates of patients with complete clinical response or without complete clinical response at each assessment. We analysed both the overall trial population and a subgroup of patients who had attended each of the three assessments by modified intention-to-treat. This study is registered at controlled-trials.com, ISRCTN 26715889.
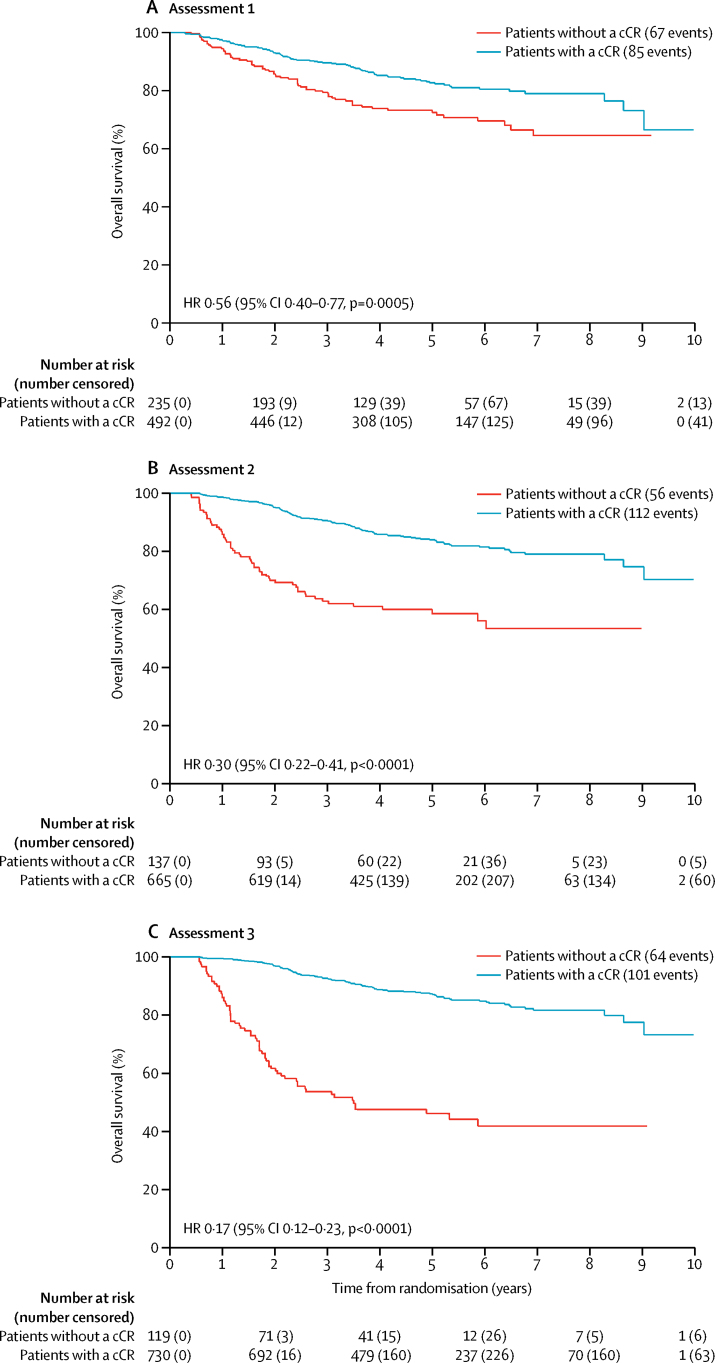
We enrolled 940 patients from June 4, 2001, until Dec 16, 2008. Complete clinical response was achieved in 492 (52%) of 940 patients at assessment 1 (11 weeks), 665 (71%) of patients at assessment 2 (18 weeks), and 730 (78%) of patients at assessment 3 (26 weeks). 691 patients attended all three assessments and in this subgroup, complete clinical response was reported in 441 (64%) patients at assessment 1, 556 (80%) at assessment 2, and 590 (85%) at assessments 3. 151 (72%) of the 209 patients who had not had a complete clinical response at assessment 1 had a complete clinical response by assessment 3. In the overall trial population of 940 patients, 5 year overall survival in patients who had a clinical response at assessments 1, 2, 3 was 83% (95% CI 79-86), 84% (81-87), and 87% (84-89), respectively and was 72% (66-78), 59% (49-67), and 46% (37-55) for patients who did not have a complete clinical response at assessments 1, 2, 3, respectively. In the subgroup of 691 patients, 5 year overall survival in patients who had a clinical response at assessment 1, 2, 3 was 85% (81-88), 86% (82-88), and 87% (84-90), respectively, and was 75% (68-80), 61% (50-70), and 48% (36-58) for patients who did not have a complete clinical response at assessment 1, 2, 3, respectively. Similarly, progression-free survival in both the overall trial population and the subgroup was longer in patients who had a complete clinical response, compared with patients who did not have a complete clinical response, at all three assessments.
Many patients who do not have a complete clinical response when assessed at 11 weeks after commencing chemoradiotherapy do in fact respond by 26 weeks, and the earlier assessment could lead to some patients having unnecessary surgery. Our data suggests that the optimum time for assessment of complete clinical response after chemoradiotherapy for patients with squamous cell carcinoma of the anus is 26 weeks from starting chemoradiotherapy. We suggest that guidelines should be revised to indicate that later assessment is acceptable.
Cancer Research UK.
肛管癌治疗指南建议在开始治疗后6 - 12周评估反应情况。我们利用ACT II试验的数据,确定了放化疗后评估临床肿瘤反应的最佳时间点。
先前报道的ACT II试验是一项3期随机试验,纳入了来自英国59个中心的新诊断、组织学确诊、无转移性疾病的各年龄段肛管鳞状细胞癌患者。我们通过最小化法将患者随机分配,分别接受静脉注射丝裂霉素(第1天12 mg/m²一剂)或静脉注射顺铂(第1天和第29天各60 mg/m²一剂),同时静脉注射氟尿嘧啶(第1 - 4天和第29 - 32天每天1000 mg/m²一剂)及放疗(28次每日分割剂量共50.4 Gy);初始治疗后还进行了第二次随机分组,分为维持化疗(氟尿嘧啶和顺铂)或不进行维持化疗。主要结局是完全临床缓解(临床检查时原发肿瘤和区域淋巴结均消失),以及自随机分组起的总生存期和无进展生存期。在这项事后分析中,我们分析了三个时间点的完全临床缓解情况:放化疗开始后11周(评估1)、18周(评估2)和26周(评估3),以及每次评估时达到完全临床缓解或未达到完全临床缓解患者的总生存期和无进展生存期估计值。我们对整个试验人群以及通过改良意向性分析参加了所有三次评估的患者亚组进行了分析。本研究已在controlled - trials.com注册,ISRCTN 26715889。
我们从2001年6月4日至2008年12月16日共纳入940例患者。在评估1(11周)时,940例患者中有492例(52%)达到完全临床缓解;评估2(18周)时,665例(71%)患者达到完全临床缓解;评估3(26周)时,730例(78%)患者达到完全临床缓解。691例患者参加了所有三次评估,在该亚组中,评估1时441例(64%)患者达到完全临床缓解,评估2时556例(80%)患者达到完全临床缓解,评估3时590例(85%)患者达到完全临床缓解。在评估1时未达到完全临床缓解的209例患者中,151例(72%)在评估3时达到完全临床缓解。在940例患者的整个试验人群中,在评估1、2、3时出现临床缓解的患者5年总生存率分别为83%(95%CI 79 - 86)、84%(81 - 87)和87%(84 - 89),而在评估1、2、3时未达到完全临床缓解的患者5年总生存率分别为72%(66 - 78)、59%(49 - 67)和46%(37 - 55)。在691例患者的亚组中,在评估1、2、3时出现临床缓解的患者5年总生存率分别为85%(81 - 88)、86%(82 - 88)和87%(84 - 90),而在评估1、2、3时未达到完全临床缓解的患者5年总生存率分别为75%(68 - 80)、61%((50 - 70)和48%(36 - 58)。同样,在所有三次评估中,整个试验人群和亚组中达到完全临床缓解的患者的无进展生存期均长于未达到完全临床缓解的患者。
许多在放化疗开始后11周评估时未达到完全临床缓解的患者实际上在26周时出现了缓解,早期评估可能导致一些患者接受不必要的手术。我们的数据表明,肛管鳞状细胞癌患者放化疗后评估完全临床缓解的最佳时间是放化疗开始后26周(182天)。我们建议修订指南,表明后期评估是可以接受的。
英国癌症研究中心。