Hiemstra Laurie A, Kerslake Sarah, Lafave Mark
Banff Sport Medicine, Banff, Alberta, Canada.; Department of Surgery, University of Calgary, Calgary, Alberta, Canada.
Banff Sport Medicine, Banff, Alberta, Canada.; Department of Physical Therapy, University of Alberta, Edmonton, Alberta, Canada.
Orthop J Sports Med. 2017 Feb 7;5(2):2325967116687749. doi: 10.1177/2325967116687749. eCollection 2017 Feb.
Medial patellofemoral ligament (MPFL) reconstruction is a procedure aimed to reestablish the checkrein to lateral patellar translation in patients with symptomatic patellofemoral instability. Correct femoral tunnel position is thought to be crucial to successful MPFL reconstruction, but the accuracy of this statement in terms of patient outcomes has not been tested.
To assess the accuracy of femoral tunnel placement in an MPFL reconstruction cohort and to determine the correlation between tunnel accuracy and a validated disease-specific, patient-reported quality-of-life outcome measure.
Case series; Level of evidence, 4.
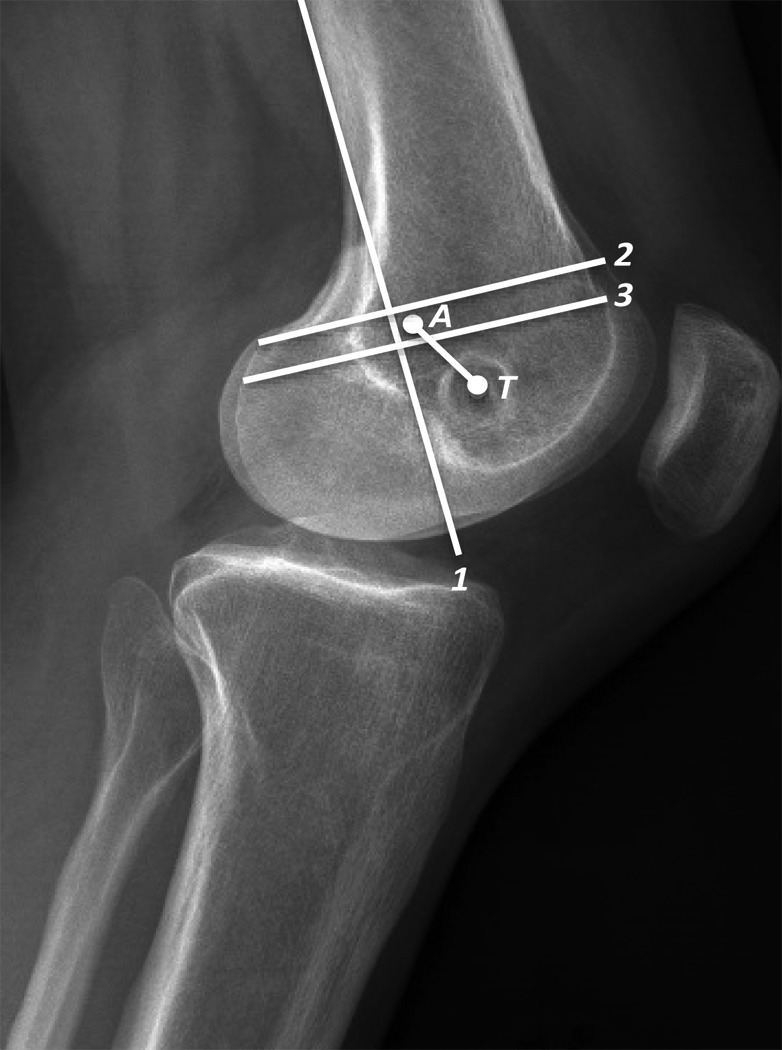
Between June 2008 and February 2014, a total of 206 subjects underwent an MPFL reconstruction. Lateral radiographs were measured to determine the accuracy of the femoral tunnel by measuring the distance from the center of the femoral tunnel to the Schöttle point. Banff Patella Instability Instrument (BPII) scores were collected a mean 24 months postoperatively.
A total of 155 (79.5%) subjects had adequate postoperative lateral radiographs and complete BPII scores. The mean duration of follow-up (±SD) was 24.4 ± 8.2 months (range, 12-74 months). Measurement from the center of the femoral tunnel to the Schöttle point resulted in 143 (92.3%) tunnels being categorized as "good" or "ideal." There were 8 failures in the cohort, none of which occurred in malpositioned tunnels. The mean distance from the center of the MPFL tunnel to the center of the Schöttle point was 5.9 ± 4.2 mm (range, 0.5-25.9 mm). The mean postoperative BPII score was 65.2 ± 22.5 (range, 9.2-100). Pearson correlation demonstrated no statistically significant relationship between accuracy of femoral tunnel position and BPII score ( = -0.08; 95% CI, -0.24 to 0.08).
There was no evidence of a correlation between the accuracy of MPFL reconstruction femoral tunnel in relation to the Schöttle point and disease-specific quality-of-life scores. Graft failure was not related to femoral tunnel placement. The patellofemoral instability population is complex, and patients present with multiple risk factors that, in addition to the accuracy of femoral tunnel position, contribute to quality of life and warrant further investigation.
髌股内侧韧带(MPFL)重建手术旨在为有症状的髌股关节不稳患者重建防止髌骨向外侧移位的制约机制。正确的股骨隧道位置被认为是MPFL重建成功的关键,但这一说法在患者预后方面的准确性尚未得到验证。
评估MPFL重建队列中股骨隧道置入的准确性,并确定隧道准确性与经过验证的疾病特异性、患者报告的生活质量结局指标之间的相关性。
病例系列;证据等级,4级。
2008年6月至2014年2月期间,共有206名受试者接受了MPFL重建手术。通过测量股骨隧道中心到朔特勒点的距离,利用侧位X线片来确定股骨隧道的准确性。术后平均24个月收集班夫髌骨不稳器械(BPII)评分。
共有155名(79.5%)受试者术后有足够的侧位X线片且BPII评分完整。平均随访时间(±标准差)为24.4±8.2个月(范围12 - 74个月)。从股骨隧道中心到朔特勒点的测量结果显示,143个(92.3%)隧道被归类为“良好”或“理想”。该队列中有8例失败病例,其中没有一例发生在位置不当的隧道中。MPFL隧道中心到朔特勒点中心的平均距离为5.9±4.2毫米(范围0.5 - 25.9毫米)。术后BPII评分的平均值为65.2±22.5(范围9.2 - 100)。Pearson相关性分析表明,股骨隧道位置的准确性与BPII评分之间无统计学显著相关性(r = -0.08;95%置信区间,-0.24至0.08)。
没有证据表明MPFL重建股骨隧道相对于朔特勒点的准确性与疾病特异性生活质量评分之间存在相关性。移植物失败与股骨隧道置入无关。髌股关节不稳人群情况复杂,患者存在多种风险因素,除了股骨隧道位置的准确性外,这些因素也会影响生活质量,值得进一步研究。