Liang Laurel, Bernhardsson Susanne, Vernooij Robin W M, Armstrong Melissa J, Bussières André, Brouwers Melissa C, Gagliardi Anna R
University of Toronto, Toronto, Canada.
Närhälsan Research and Development Centre for Primary Health Care, Region Västra Götaland, Göteborg, Sweden.
Implement Sci. 2017 Feb 27;12(1):26. doi: 10.1186/s13012-017-0557-0.
Guidelines support health care decision-making and high quality care and outcomes. However, their implementation is sub-optimal. Theory-informed, tailored implementation is associated with guideline use. Few guideline implementation studies published up to 1998 employed theory. This study aimed to describe if and how theory is now used to plan or evaluate guideline implementation among physicians.
A scoping review was conducted. MEDLINE, EMBASE, and The Cochrane Library were searched from 2006 to April 2016. English language studies that planned or evaluated guideline implementation targeted to physicians based on explicitly named theory were eligible. Screening and data extraction were done in duplicate. Study characteristics and details about theory use were analyzed.
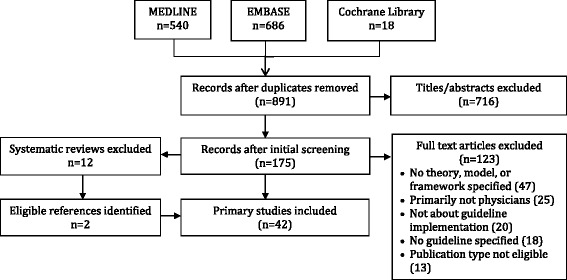
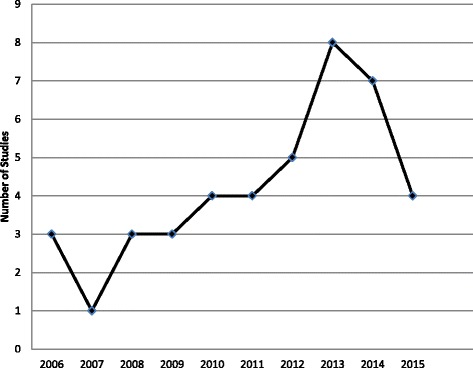
A total of 1244 published reports were identified, 891 were unique, and 716 were excluded based on title and abstract. Among 175 full-text articles, 89 planned or evaluated guideline implementation targeted to physicians; 42 (47.2%) were based on theory and included. The number of studies using theory increased yearly and represented a wide array of countries, guideline topics and types of physicians. The Theory of Planned Behavior (38.1%) and the Theoretical Domains Framework (23.8%) were used most frequently. Many studies rationalized choice of theory (83.3%), most often by stating that the theory described implementation or its determinants, but most failed to explicitly link barriers with theoretical constructs. The majority of studies used theory to inform surveys or interviews that identified barriers of guideline use as a preliminary step in implementation planning (76.2%). All studies that evaluated interventions reported positive impact on reported physician or patient outcomes.
While the use of theory to design or evaluate interventions appears to be increasing over time, this review found that one half of guideline implementation studies were based on theory and many of those provided scant details about how theory was used. This limits interpretation and replication of those interventions, and seems to result in multifaceted interventions, which may not be feasible outside of scientific investigation. Further research is needed to better understand how to employ theory in guideline implementation planning or evaluation.
指南有助于医疗保健决策以及提供高质量的医疗服务和成果。然而,其实施情况并不理想。基于理论且经过量身定制的实施方式与指南的使用相关。截至1998年,已发表的指南实施研究中很少有运用理论的。本研究旨在描述如今是否以及如何运用理论来规划或评估医生对指南的实施情况。
进行了一项范围综述。检索了2006年至2016年4月期间的MEDLINE、EMBASE和考克兰图书馆。纳入基于明确提及的理论、针对医生规划或评估指南实施情况的英文研究。筛选和数据提取由两人独立进行。分析了研究特征以及有关理论运用的细节。
共识别出1244篇已发表报告,其中891篇为独立报告,根据标题和摘要排除了716篇。在175篇全文文章中,89篇针对医生规划或评估了指南实施情况;42篇(47.2%)基于理论并被纳入。运用理论的研究数量逐年增加,涉及众多国家、指南主题和医生类型。计划行为理论(38.1%)和理论领域框架(23.8%)使用最为频繁。许多研究为理论的选择提供了理由(83.3%),最常见的理由是该理论描述了实施情况或其决定因素,但大多数研究未能明确将障碍与理论结构联系起来。大多数研究运用理论为调查或访谈提供信息,这些调查或访谈将指南使用的障碍识别为实施规划的初步步骤(76.2%)。所有评估干预措施的研究均报告了对医生或患者报告结局的积极影响。
虽然随着时间推移,运用理论设计或评估干预措施的情况似乎在增加,但本综述发现,一半的指南实施研究基于理论,其中许多研究关于理论如何运用的细节很少。这限制了对这些干预措施的解释和复制,似乎导致了多方面的干预措施,而这些措施在科学研究之外可能并不可行。需要进一步研究以更好地理解如何在指南实施规划或评估中运用理论。