Spika Devon, Bannon Finian, Bonaventure Audrey, Woods Laura M, Harewood Rhea, Carreira Helena, Coleman Michel P, Allemani Claudia
Cancer Survival Group, Department of Non-Communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine, Keppel Street, London, WC1E 7HT, UK.
Centre for Public Health, Queens University Belfast, Institute of Clinical Sciences, Block B, Grosvenor Road, Belfast, BT12 6BA, UK.
BMC Cancer. 2017 Feb 27;17(1):159. doi: 10.1186/s12885-017-3117-8.
We set out to estimate net survival trends for 10 common cancers in 279 cancer registry populations in 67 countries around the world, as part of the CONCORD-2 study. Net survival can be interpreted as the proportion of cancer patients who survive up to a given time, after eliminating the impact of mortality from other causes (background mortality). Background mortality varies widely between populations and over time. It was therefore necessary to construct robust life tables that accurately reflected the background mortality in each of the registry populations.
Life tables of all-cause mortality rates by single year of age and sex were constructed by calendar year for each population and, when possible, by racial or ethnic sub-groups. We used three different approaches, based on the type of mortality data available from each registry. With death and population counts, we adopted a flexible multivariable modelling approach. With unsmoothed mortality rates, we used the Ewbank relational method. Where no data were available from the registry or a national statistical office, we used the abridged UN Population Division life tables and interpolated these using the Elandt-Johnson method. We also investigated the impact of using state- and race-specific life tables versus national race-specific life tables on estimates of net survival from four adult cancers in the United States (US).
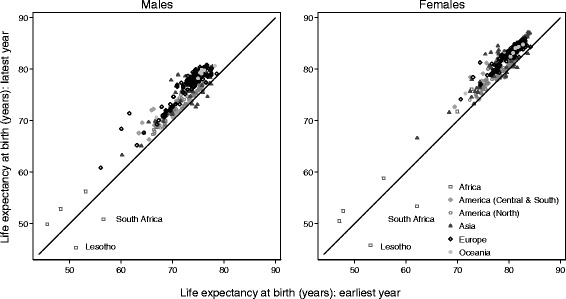
We constructed 6,514 life tables covering 327 populations. Wide variations in life expectancy at birth and mortality by age were observed, even within countries. During 1995-99, life expectancy was lowest in Nigeria and highest in Japan, ranging from 47 to 84 years among females and 46 to 78 years among males. During 2005-09, life expectancy was lowest in Lesotho and again highest in Japan, ranging from 45 to 86 years among females and 45 to 80 years among males. For the US, estimates of net survival differed by up to 4% if background mortality was fully controlled with state- and race-specific life tables, rather than with national race-specific life tables.
Background mortality varies worldwide. This emphasises the importance of using population-specific life tables for geographic and international comparisons of net survival.
作为CONCORD-2研究的一部分,我们着手估计全球67个国家279个癌症登记处人群中10种常见癌症的净生存趋势。净生存可解释为在消除其他原因(背景死亡率)导致的死亡影响后,存活至特定时间的癌症患者比例。背景死亡率在不同人群之间以及随时间变化差异很大。因此,有必要构建能准确反映每个登记处人群背景死亡率的稳健生命表。
按历年为每个人口群体构建按单一年龄和性别划分的全因死亡率生命表,可能的话还按种族或族裔亚组构建。根据每个登记处可得的死亡率数据类型,我们采用了三种不同方法。对于有死亡人数和人口数的情况,我们采用灵活的多变量建模方法。对于未平滑的死亡率,我们使用埃温克关系法。在登记处或国家统计局没有数据的地方,我们使用联合国人口司简略生命表,并采用埃兰特 - 约翰逊方法进行插值。我们还研究了在美国使用州和种族特定生命表与国家种族特定生命表对四种成人癌症净生存估计的影响。
我们构建了涵盖327个人口群体的6514个生命表。即使在国家内部,也观察到出生时预期寿命和年龄别死亡率存在很大差异。在1995 - 1999年期间,尼日利亚的预期寿命最低,日本最高,女性为47至84岁,男性为46至78岁。在2005 - 2009年期间,莱索托的预期寿命最低,日本再次最高,女性为45至86岁,男性为45至80岁。对于美国,如果用州和种族特定生命表而不是国家种族特定生命表来完全控制背景死亡率,净生存估计值相差高达4%。
背景死亡率在全球范围内各不相同。这凸显了在进行净生存的地理和国际比较时使用特定人群生命表的重要性。