Lancet. 2024 May 18;403(10440):1989-2056. doi: 10.1016/S0140-6736(24)00476-8. Epub 2024 Mar 11.
Estimates of demographic metrics are crucial to assess levels and trends of population health outcomes. The profound impact of the COVID-19 pandemic on populations worldwide has underscored the need for timely estimates to understand this unprecedented event within the context of long-term population health trends. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2021 provides new demographic estimates for 204 countries and territories and 811 additional subnational locations from 1950 to 2021, with a particular emphasis on changes in mortality and life expectancy that occurred during the 2020-21 COVID-19 pandemic period.
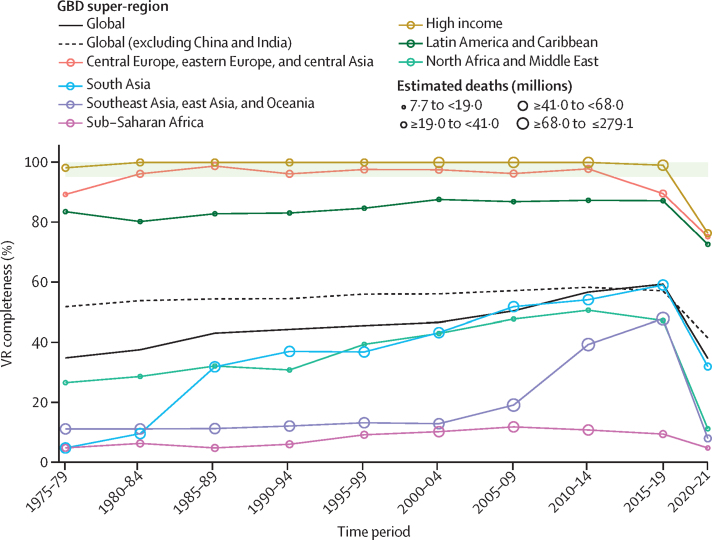
22 223 data sources from vital registration, sample registration, surveys, censuses, and other sources were used to estimate mortality, with a subset of these sources used exclusively to estimate excess mortality due to the COVID-19 pandemic. 2026 data sources were used for population estimation. Additional sources were used to estimate migration; the effects of the HIV epidemic; and demographic discontinuities due to conflicts, famines, natural disasters, and pandemics, which are used as inputs for estimating mortality and population. Spatiotemporal Gaussian process regression (ST-GPR) was used to generate under-5 mortality rates, which synthesised 30 763 location-years of vital registration and sample registration data, 1365 surveys and censuses, and 80 other sources. ST-GPR was also used to estimate adult mortality (between ages 15 and 59 years) based on information from 31 642 location-years of vital registration and sample registration data, 355 surveys and censuses, and 24 other sources. Estimates of child and adult mortality rates were then used to generate life tables with a relational model life table system. For countries with large HIV epidemics, life tables were adjusted using independent estimates of HIV-specific mortality generated via an epidemiological analysis of HIV prevalence surveys, antenatal clinic serosurveillance, and other data sources. Excess mortality due to the COVID-19 pandemic in 2020 and 2021 was determined by subtracting observed all-cause mortality (adjusted for late registration and mortality anomalies) from the mortality expected in the absence of the pandemic. Expected mortality was calculated based on historical trends using an ensemble of models. In location-years where all-cause mortality data were unavailable, we estimated excess mortality rates using a regression model with covariates pertaining to the pandemic. Population size was computed using a Bayesian hierarchical cohort component model. Life expectancy was calculated using age-specific mortality rates and standard demographic methods. Uncertainty intervals (UIs) were calculated for every metric using the 25th and 975th ordered values from a 1000-draw posterior distribution.
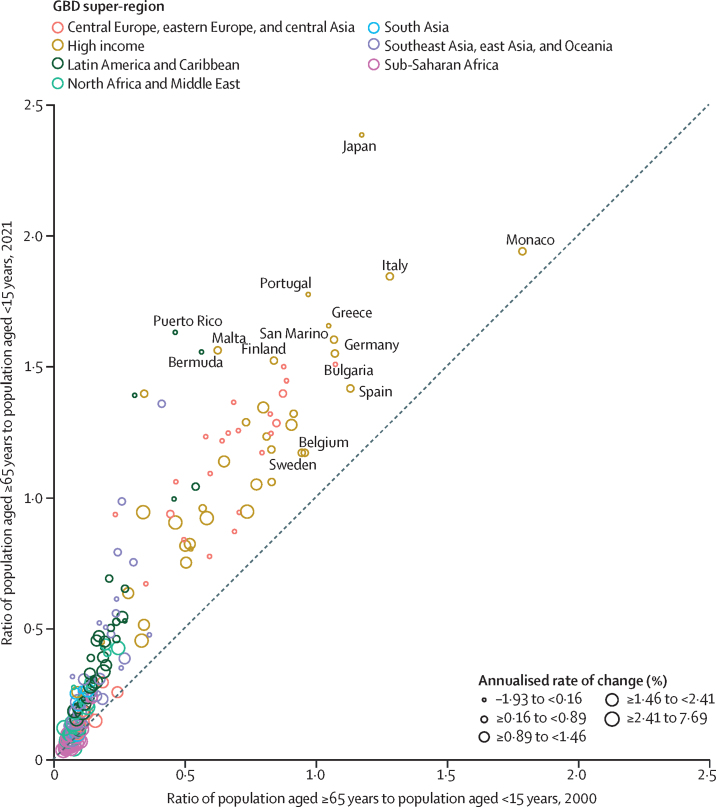
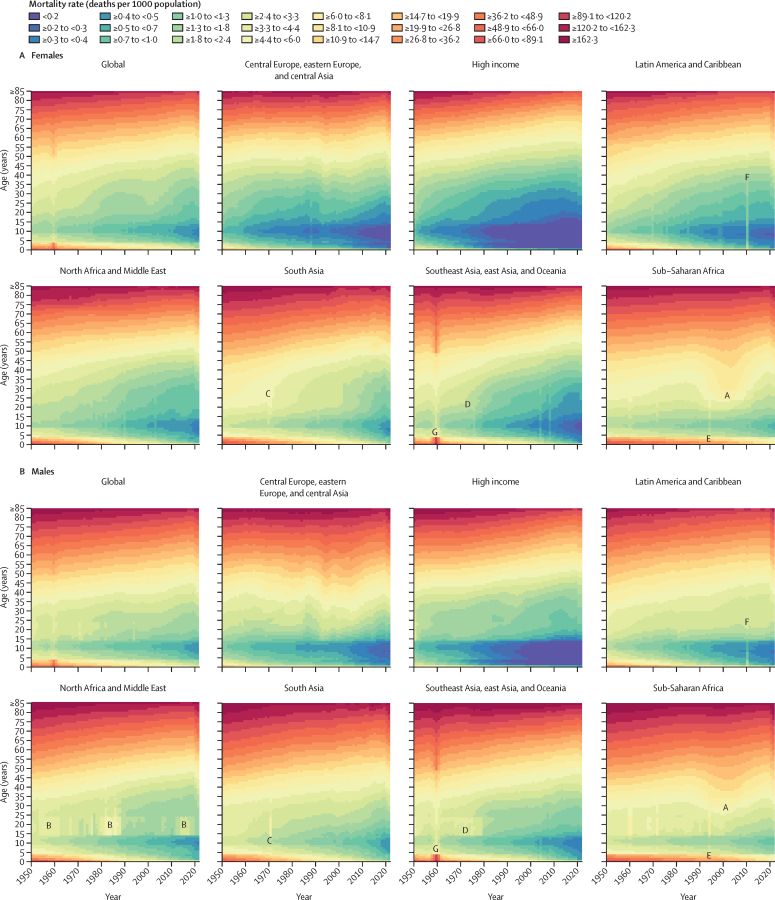
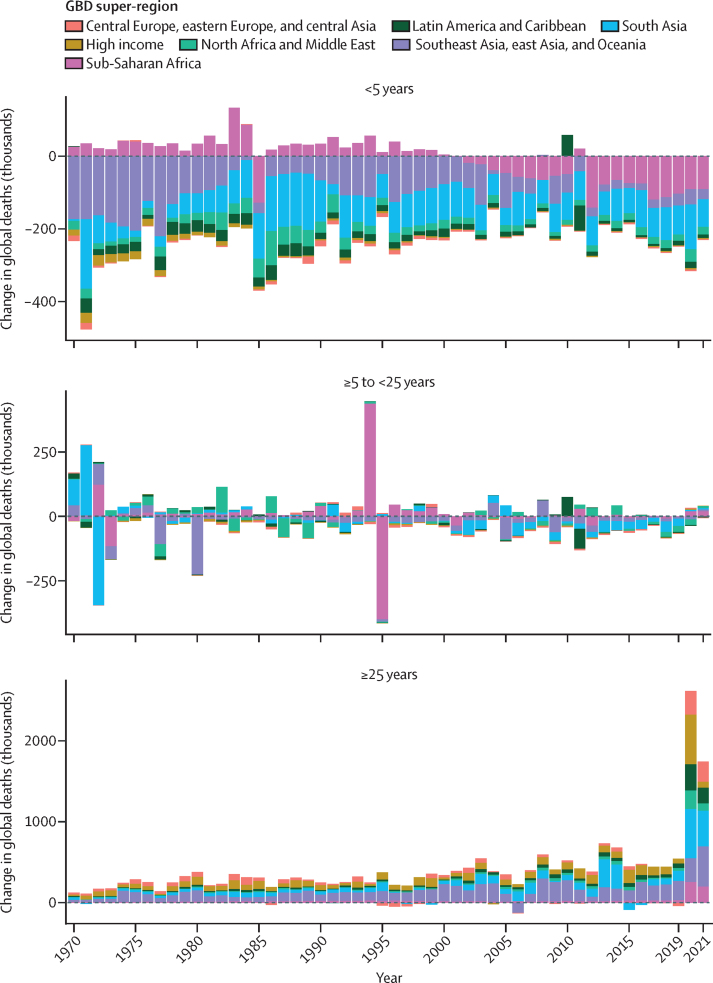
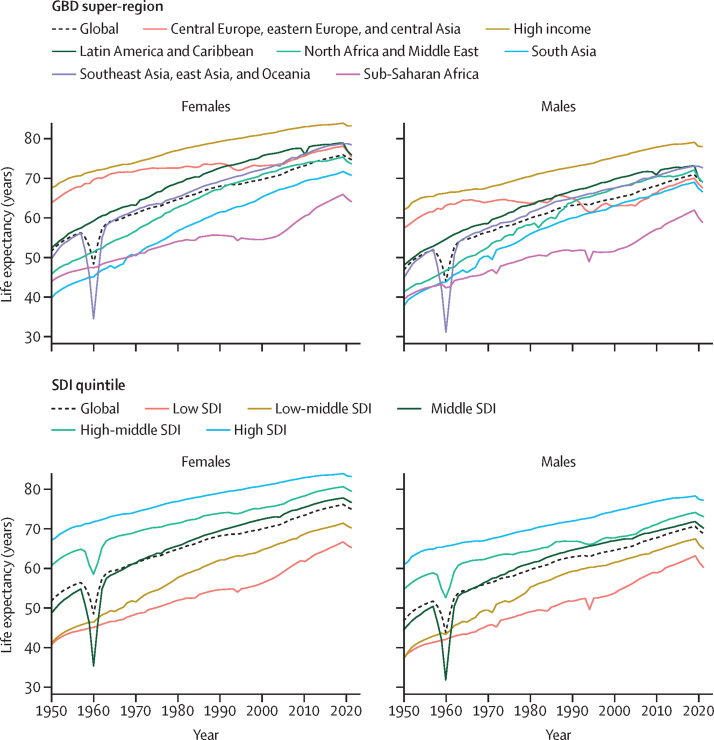
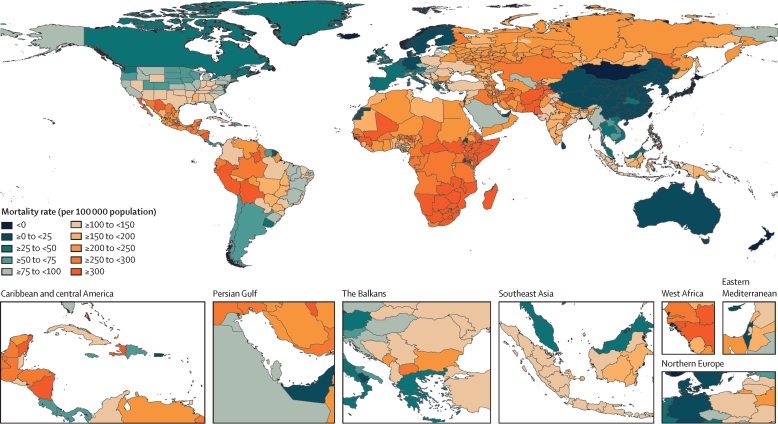
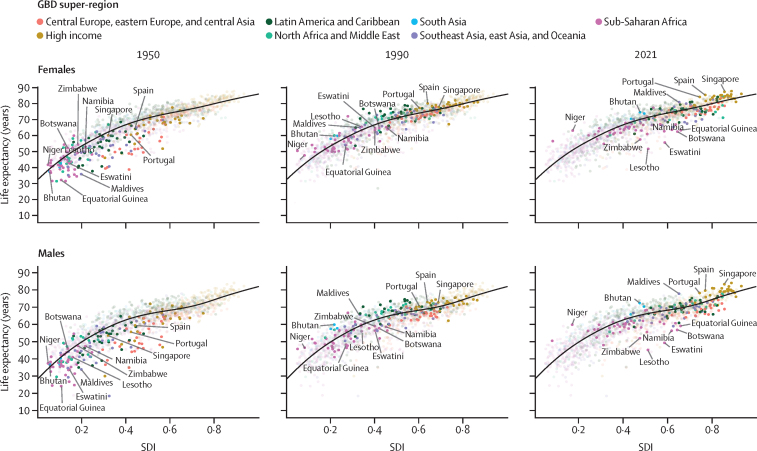
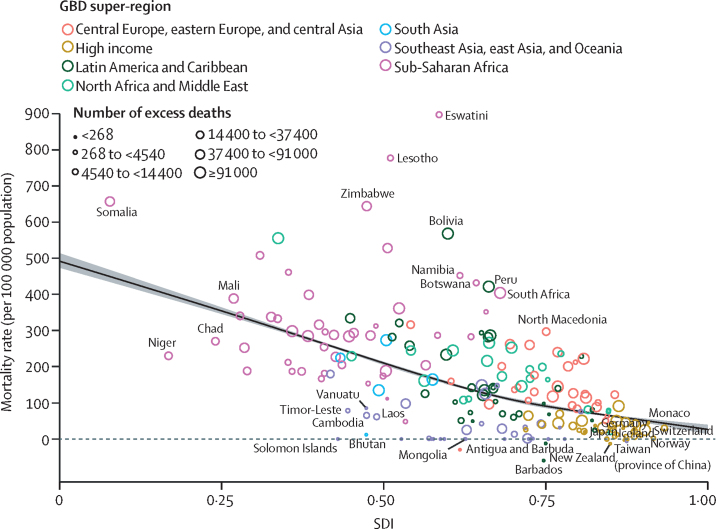
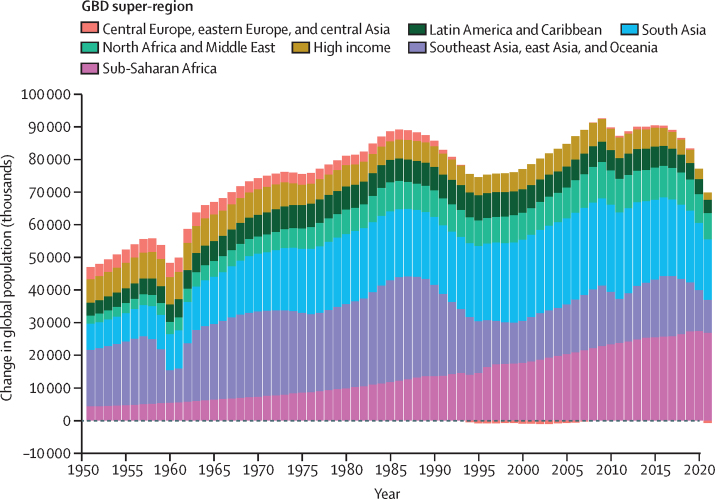
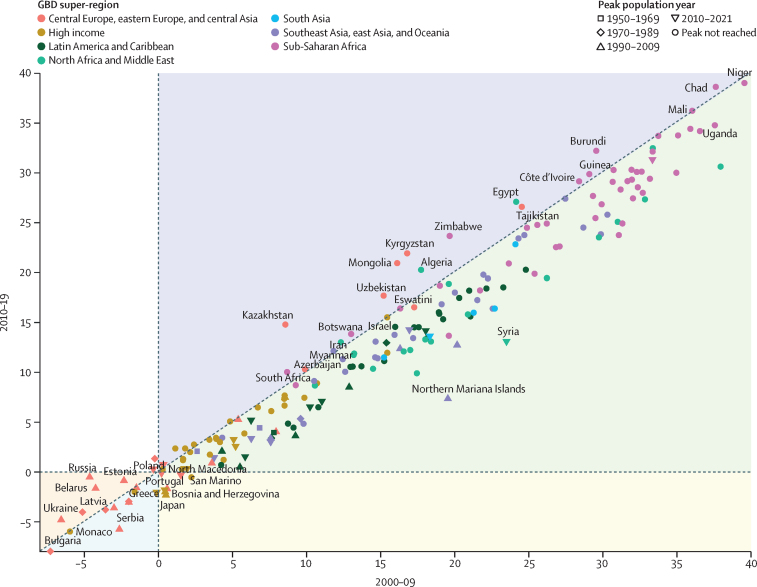
Global all-cause mortality followed two distinct patterns over the study period: age-standardised mortality rates declined between 1950 and 2019 (a 62·8% [95% UI 60·5-65·1] decline), and increased during the COVID-19 pandemic period (2020-21; 5·1% [0·9-9·6] increase). In contrast with the overall reverse in mortality trends during the pandemic period, child mortality continued to decline, with 4·66 million (3·98-5·50) global deaths in children younger than 5 years in 2021 compared with 5·21 million (4·50-6·01) in 2019. An estimated 131 million (126-137) people died globally from all causes in 2020 and 2021 combined, of which 15·9 million (14·7-17·2) were due to the COVID-19 pandemic (measured by excess mortality, which includes deaths directly due to SARS-CoV-2 infection and those indirectly due to other social, economic, or behavioural changes associated with the pandemic). Excess mortality rates exceeded 150 deaths per 100 000 population during at least one year of the pandemic in 80 countries and territories, whereas 20 nations had a negative excess mortality rate in 2020 or 2021, indicating that all-cause mortality in these countries was lower during the pandemic than expected based on historical trends. Between 1950 and 2021, global life expectancy at birth increased by 22·7 years (20·8-24·8), from 49·0 years (46·7-51·3) to 71·7 years (70·9-72·5). Global life expectancy at birth declined by 1·6 years (1·0-2·2) between 2019 and 2021, reversing historical trends. An increase in life expectancy was only observed in 32 (15·7%) of 204 countries and territories between 2019 and 2021. The global population reached 7·89 billion (7·67-8·13) people in 2021, by which time 56 of 204 countries and territories had peaked and subsequently populations have declined. The largest proportion of population growth between 2020 and 2021 was in sub-Saharan Africa (39·5% [28·4-52·7]) and south Asia (26·3% [9·0-44·7]). From 2000 to 2021, the ratio of the population aged 65 years and older to the population aged younger than 15 years increased in 188 (92·2%) of 204 nations.
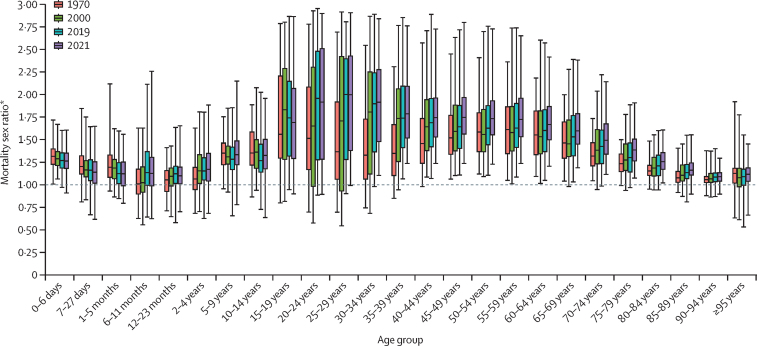
Global adult mortality rates markedly increased during the COVID-19 pandemic in 2020 and 2021, reversing past decreasing trends, while child mortality rates continued to decline, albeit more slowly than in earlier years. Although COVID-19 had a substantial impact on many demographic indicators during the first 2 years of the pandemic, overall global health progress over the 72 years evaluated has been profound, with considerable improvements in mortality and life expectancy. Additionally, we observed a deceleration of global population growth since 2017, despite steady or increasing growth in lower-income countries, combined with a continued global shift of population age structures towards older ages. These demographic changes will likely present future challenges to health systems, economies, and societies. The comprehensive demographic estimates reported here will enable researchers, policy makers, health practitioners, and other key stakeholders to better understand and address the profound changes that have occurred in the global health landscape following the first 2 years of the COVID-19 pandemic, and longer-term trends beyond the pandemic.
Bill & Melinda Gates Foundation.
人口统计指标的估计对于评估人口健康结果的水平和趋势至关重要。COVID-19 大流行对全球人口的深远影响突显了及时进行估计的必要性,以便在长期人口健康趋势的背景下了解这一前所未有的事件。全球疾病、伤害和危险因素研究(GBD)2021 年提供了 204 个国家和地区以及 811 个额外的次国家地点从 1950 年到 2021 年的新人口统计数据估计,特别强调了 2020-21 年 COVID-19 大流行期间发生的死亡率和预期寿命的变化。
使用 22223 个来自生命登记、样本登记、调查、人口普查和其他来源的数据估计死亡率,其中一部分数据源专门用于估计 COVID-19 大流行期间由于该疾病而导致的超额死亡率。2026 年的数据用于人口估计。其他来源用于估计移民;艾滋病毒流行的影响;以及冲突、饥荒、自然灾害和大流行造成的人口统计不连续,这些都被用作估计死亡率和人口的输入。时空高斯过程回归(ST-GPR)用于生成 5 岁以下儿童死亡率,该死亡率综合了 30763 个地点年份的生命登记和样本登记数据、1365 次调查和人口普查以及 80 个其他来源的数据。ST-GPR 还用于根据 31642 个地点年份的生命登记和样本登记数据、355 次调查和人口普查以及 24 个其他来源的数据来估计 15-59 岁成年人的死亡率。然后,使用关系模型生命表系统生成儿童和成年人死亡率的生命表。对于 HIV 流行较大的国家,使用通过对 HIV 流行率调查、产前诊所血清学监测和其他数据源进行的 HIV 特异性死亡率的流行病学分析生成的独立 HIV 特定死亡率估计来调整生命表。通过减去调整后所有原因死亡率(考虑了晚期登记和死亡率异常)与大流行期间不存在大流行时的死亡率,确定 2020 年和 2021 年 COVID-19 大流行期间的超额死亡率。预期死亡率是根据历史趋势使用基于模型的集合计算得出的。在所有原因死亡率数据不可用的地点年份,我们使用与大流行相关的协变量回归模型来估计超额死亡率率。人口规模使用贝叶斯分层队列分量模型计算。使用标准人口统计学方法计算预期寿命。使用来自 1000 次后验分布的第 25 和第 975 个有序值为每个指标计算不确定区间(UI)。
在研究期间,全球所有原因死亡率呈现出两种截然不同的模式:1950 年至 1999 年期间年龄标准化死亡率下降(62.8%[95%UI 60.5-65.1]下降),而 COVID-19 大流行期间增加(2020-21 年;5.1%[0.9-9.6]增加)。与大流行期间死亡率趋势的总体逆转形成鲜明对比的是,儿童死亡率继续下降,2021 年 5 岁以下儿童全球死亡人数为 466 万(398-550),而 2019 年为 521 万(450-601)。据估计,2020 年和 2021 年全球共有 1.31 亿人死于各种原因,其中 1590 万人(1470-1720)是 COVID-19 大流行所致(通过超额死亡率衡量,包括直接死于 SARS-CoV-2 感染的死亡人数和与大流行相关的其他社会、经济或行为变化导致的间接死亡人数)。在 80 个国家和地区,至少有一年的大流行期间,超额死亡率率超过每 10 万人 150 人死亡,而 2020 年或 2021 年有 20 个国家的超额死亡率率为负,这表明这些国家的全因死亡率在大流行期间低于历史趋势预期。1950 年至 2021 年期间,全球出生时预期寿命增加了 22.7 岁(20.8-24.8),从 49.0 岁(46.7-51.3)增加到 71.7 岁(70.9-72.5)。2019 年至 2021 年期间,全球出生时预期寿命下降了 1.6 岁(1.0-2.2),扭转了历史趋势。在 2019 年至 2021 年期间,仅在 32 个(15.7%)204 个国家和地区观察到预期寿命的增加。2021 年全球人口达到 78.9 亿(76.7-81.3),此时 204 个国家和地区中有 56 个达到峰值,此后人口下降。2020 年至 2021 年期间,人口增长最大的是撒哈拉以南非洲(39.5%[28.4-52.7])和南亚(26.3%[9.0-44.7])。从 2000 年到 2021 年,65 岁及以上人口与 15 岁以下人口之比在 204 个国家中的 188 个(92.2%)增加。
2020 年和 2021 年 COVID-19 大流行期间,全球成人死亡率显著上升,扭转了过去的下降趋势,而儿童死亡率虽然下降速度较前几年有所放缓,但仍在继续。尽管 COVID-19 在大流行的头两年对许多人口统计指标产生了重大影响,但在评估的 72 年中,全球健康进展总体上是深远的,死亡率和预期寿命都有了相当大的改善。此外,自 2017 年以来,我们观察到全球人口增长率放缓,尽管较低收入国家的人口增长稳定或有所增加,并且全球人口年龄结构持续向老年化转变。这些人口变化可能会给卫生系统、经济和社会带来未来的挑战。这里报告的全面人口统计估计将使研究人员、政策制定者、卫生保健从业者和其他利益攸关方能够更好地了解和应对 COVID-19 大流行头两年全球健康格局中发生的深刻变化,以及大流行以外的长期趋势。
比尔和梅琳达·盖茨基金会。