Heng Somony, Durnez Lies, Mao Sokny, Siv Sovannaroth, Tho Sochantha, Mean Vanna, Sluydts Vincent, Coosemans Marc
National Center for Parasitology, Entomology and Malaria Control, Phnom Penh, Cambodia.
Department of Biomedical Sciences, Institute of Tropical Medicine, Antwerp, Belgium.
Malar J. 2017 Mar 6;16(1):104. doi: 10.1186/s12936-017-1758-3.
Cambodia reduced malaria incidence by more than 75% between 2000 and 2015, a target of the Millennium Development Goal 6. The Cambodian Government aims to eliminate all forms of malaria by 2025. The country's malaria incidence is highly variable at provincial level, but less is known at village level. This study used passive case detection (PCD) data at village level in Ratanakiri Province from 2010 to 2014 to describe incidence trends and identify high-risk areas of malaria to be primarily targeted towards malaria elimination.
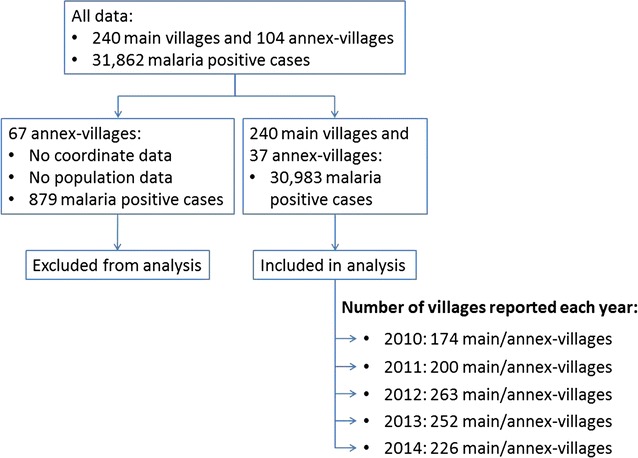
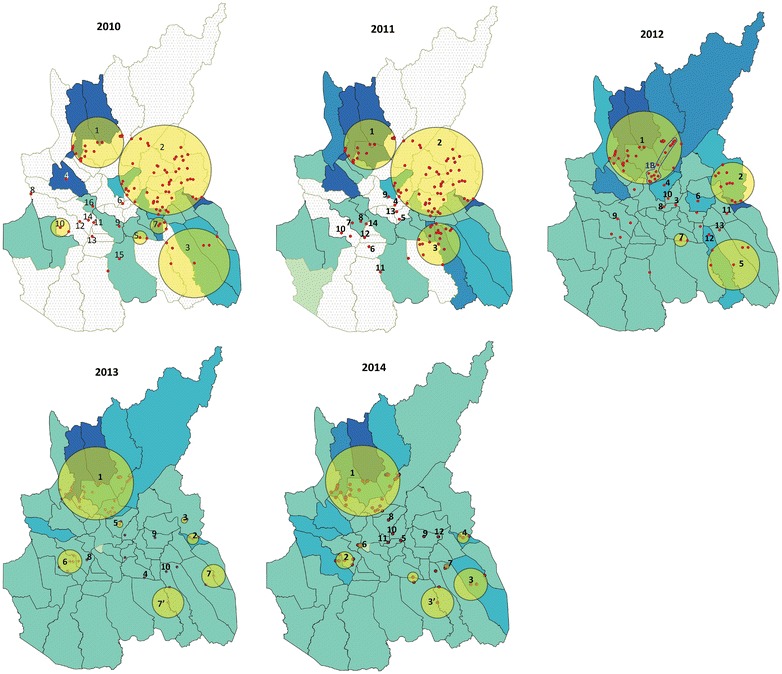
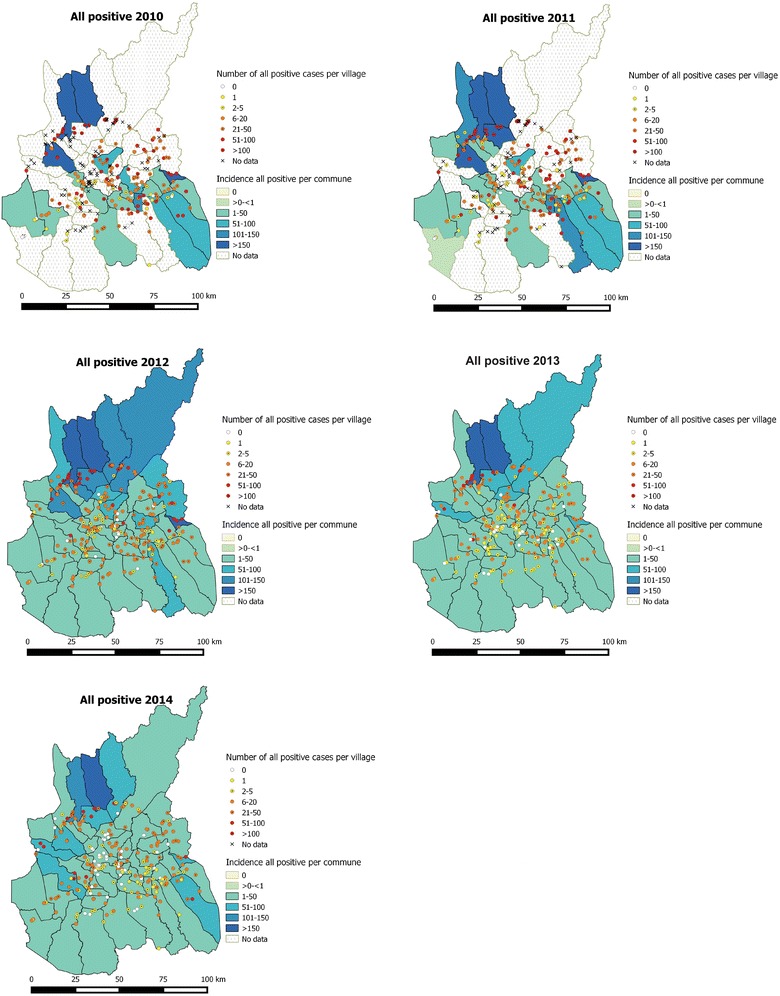
In 2010, the Cambodian malaria programme created a Malaria Information System (MIS) to capture malaria information at village level through PCD by village malaria workers and health facilities. The MIS data of Ratanakiri Province 2010-2014 were used to calculate annual incidence rates by Plasmodium species at province and commune levels. For estimating the trend at provincial level only villages reporting each year were selected. The communal incidences and the number of cases per village were visualized on a map per Plasmodium species and per year. Analysis of spatial clustering of village malaria cases by Plasmodium species was performed by year.
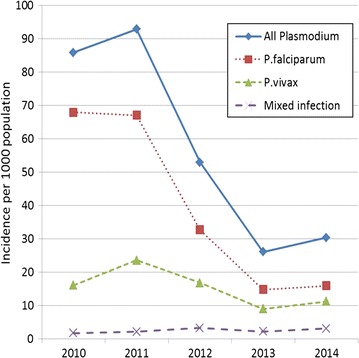
Overall, malaria annual incidence rates per 1000 inhabitants decreased from 86 (2010) to 30 (2014). Falciparum incidence decreased (by 79% in 2014 compared to 2010; CI 95% 76-82%) more rapidly than vivax incidence (by 19% in 2014 compared to 2010; CI 95% 5-32%). There were ten to 16 significant spatial clusters each year. Big clusters tended to extend along the Cambodian-Vietnamese border and along the Sesan River. Three clusters appeared throughout all years (2010-2014): one with 21 villages appeared each year, the second shrunk progressively from 2012 to 2014 and the third was split into two smaller clusters in 2013 and 2014.
The decline of malaria burden can be attributed to intensive malaria control activities implemented in the areas: distribution of a long-lasting insecticidal net per person and early diagnosis and prompt treatment. Dihydro-artemisinin piperaquine was the only first-line treatment for all malaria cases. No radical treatment with primaquine was provided for Plasmodium vivax cases, which could explain the slow decrease of P. vivax due to relapses. To achieve malaria elimination by 2025, priority should be given to the control of stable malaria clusters appearing over time.
柬埔寨在2000年至2015年间将疟疾发病率降低了75%以上,这是千年发展目标6的一项指标。柬埔寨政府旨在到2025年消除所有形式的疟疾。该国省级层面的疟疾发病率差异很大,但村级层面的情况了解较少。本研究利用2010年至2014年腊塔纳基里省村级层面的被动病例检测(PCD)数据来描述发病率趋势,并确定疟疾的高风险地区,以便主要针对这些地区开展疟疾消除工作。
2010年,柬埔寨疟疾项目创建了疟疾信息系统(MIS),通过村级疟疾防治人员和卫生设施的被动病例检测来收集村级层面的疟疾信息。利用腊塔纳基里省2010 - 2014年的MIS数据,按疟原虫种类计算省和公社层面的年发病率。仅为估算省级层面的趋势,选取了每年上报的村庄。按疟原虫种类和年份,将各公社的发病率及每个村庄的病例数绘制成地图。每年对按疟原虫种类划分的村级疟疾病例进行空间聚集性分析。
总体而言,每1000名居民的疟疾年发病率从2010年的86例降至2014年的30例。恶性疟发病率下降(2014年相较于2010年下降了79%;95%置信区间76 - 82%)比间日疟发病率下降(2014年相较于2010年下降了19%;95%置信区间5 - 32%)更为迅速。每年有10至16个显著的空间聚集区。大的聚集区往往沿着柬埔寨与越南边境以及塞桑河延伸。有三个聚集区在2010 - 2014年期间一直存在:一个每年有21个村庄,第二个从2012年到2014年逐渐缩小,第三个在2013年和2014年分裂成两个较小的聚集区。
疟疾负担的下降可归因于在这些地区开展的强化疟疾防控活动:每人分发长效驱虫蚊帐以及早期诊断和及时治疗。双氢青蒿素哌喹是所有疟疾病例的唯一一线治疗药物。间日疟病例未提供伯氨喹进行根治治疗,这可能解释了间日疟因复发导致下降缓慢的原因。为在2025年实现疟疾消除,应优先控制长期存在的稳定疟疾聚集区。