Camm A John, Accetta Gabriele, Al Mahmeed Wael, Ambrosio Giuseppe, Goldhaber Samuel Z, Haas Sylvia, Jansky Petr, Kayani Gloria, Misselwitz Frank, Oh Seil, Oto Ali, Raatikainen Pekka, Steffel Jan, van Eickels Martin, Kakkar Ajay K
St George's University of London, and Imperial College, London, UK.
Thrombosis Research Institute, London, UK.
BMJ Open. 2017 Mar 6;7(3):e014579. doi: 10.1136/bmjopen-2016-014579.
Global Anticoagulant Registry in the FIELD-Atrial Fibrillation (GARFIELD-AF) explored the impact of gender, risk factors and anticoagulant (AC) treatment on 1-year outcomes in patients with non-valvular atrial fibrillation (NVAF).
GARFIELD-AF is a prospective non-interventional registry.
Investigator sites (n=1048) are representative of the care settings/locations in each of the 35 countries.
Patients ≥18yrs with newly diagnosed (≤6 weeks' duration) NVAF and ≥1 investigator-determined stroke risk factors.
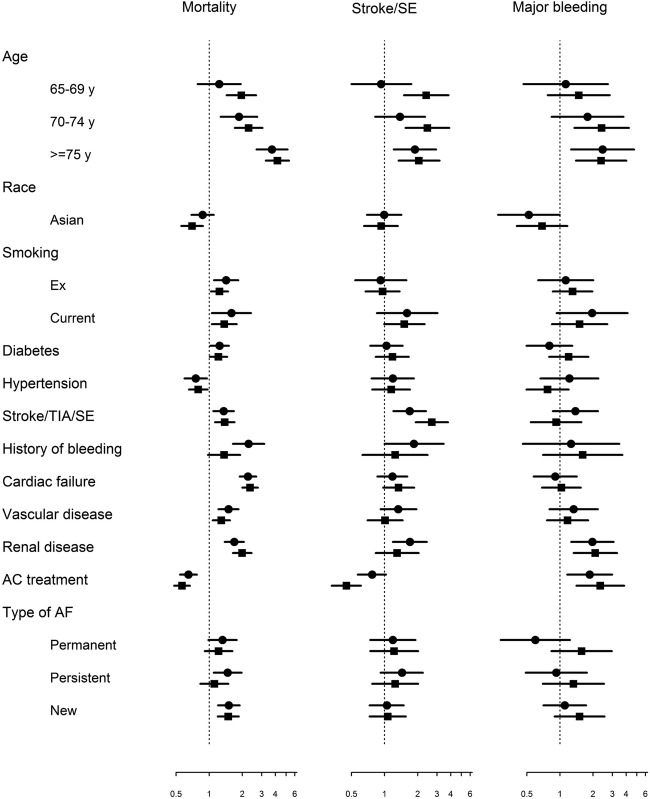
Event rates per 100 person-years were estimated from the Poisson model and HRs and 95% CIs calculated.
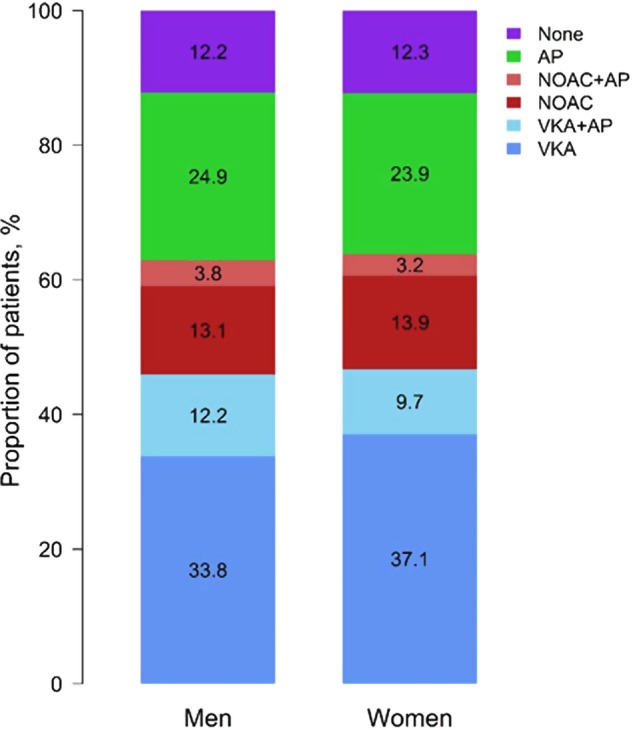
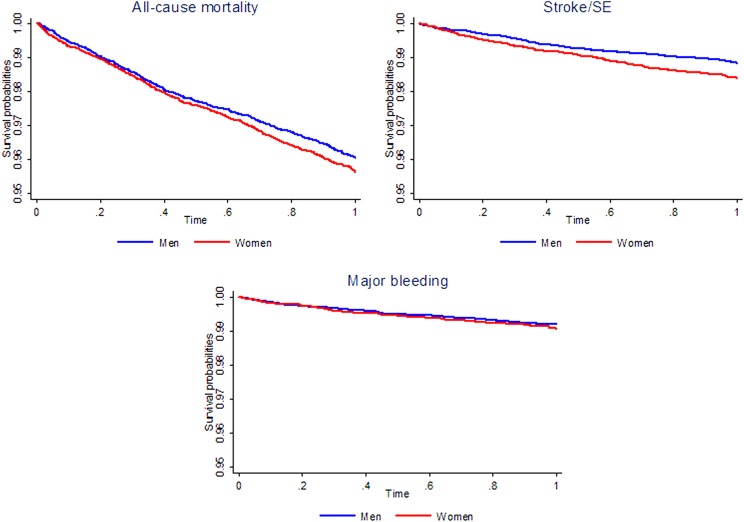
Of 28 624 patients (women 44.4%; men 55.6%) enrolled, there were more elderly (≥75 years) women (46.9%) than men (30.4%). All-cause mortality rates per 100 person-years (95% CI) for women and men were 4.48 (4.12 to 4.87) and 4.04 (3.74 to 4.38), respectively, stroke/systemic embolism (SE) (1.62 (1.41 to 1.87) and 1.17 (1.01 to 1.36)) and major bleeding (0.93 (0.78 to 1.13) and 0.79 (0.66 to 0.95)). After adjustment for baseline risk factors in treated and untreated patients, HRs (95% CI) for women (relative to men) for stroke/SE rates were 1.3-fold higher in women (HR 1.30 (1.04 to 1.63)), and similar for major bleeding (1.13 (0.85 to 1.50)) and all-cause mortality (1.05 (0.92 to 1.19)). Antithrombotic treatment patterns in men and women were almost identical. 63.8% women and 62.9% men received AC± antiplatelets. Relative to no AC treatment, the reduction in stroke/SE rates with AC treatment was greater (p=0.01) in men (HR 0.45 (0.33 to 0.61)) than women 0.77 (0.57 to 1.03). All-cause mortality reduction with AC treatment was similar (women: 0.65 (0.54 to 0.77); men: 0.57 (0.48 to 0.68)). The risk of major bleeding when treated with AC versus no AC was 2.33 (1.41 to 3.84) in men and 1.86 (1.16 to 2.99) in women (p value=0.53).
Women have a higher risk of stroke/SE and the reduction in stroke/SE events rates with AC treatment is less in women than in men.
NCT01090362.
FIELD-房颤全球抗凝登记研究(GARFIELD-AF)探讨了性别、危险因素及抗凝治疗对非瓣膜性房颤(NVAF)患者1年预后的影响。
GARFIELD-AF是一项前瞻性非干预性登记研究。
研究站点(n = 1048)代表35个国家中每个国家的医疗环境/地点。
年龄≥18岁、新诊断(病程≤6周)的NVAF患者,且有≥1个研究者确定的卒中危险因素。
通过泊松模型估计每100人年的事件发生率,并计算HR及95%CI。
纳入的28624例患者中(女性44.4%;男性55.6%),老年(≥75岁)女性(46.9%)多于男性(30.4%)。女性和男性每100人年的全因死亡率(95%CI)分别为4.48(4.12至4.87)和4.04(3.74至4.38),卒中/全身性栓塞(SE)发生率分别为1.62(1.41至1.87)和1.17(1.01至1.36),大出血发生率分别为0.93(0.78至1.13)和0.79(0.66至0.95)。在对治疗和未治疗患者的基线危险因素进行校正后,女性(相对于男性)卒中/SE发生率的HR(95%CI)高1.3倍(HR 1.30(1.04至1.63));大出血(1.13(0.85至1.50))和全因死亡率(1.05(0.92至1.19))的HR相似。男性和女性的抗栓治疗模式几乎相同。63.8%的女性和62.9%的男性接受了抗凝剂±抗血小板药物治疗。相对于未进行抗凝治疗,抗凝治疗使男性卒中/SE发生率的降低幅度更大(p = 0.01)(HR 0.45(0.33至0.61)),而女性为0.77(0.57至1.03)。抗凝治疗使全因死亡率的降低幅度相似(女性:0.65(0.54至0.77);男性:0.57(0.48至0.68))。接受抗凝治疗与未接受抗凝治疗相比,男性大出血风险为2.33(1.41至3.84),女性为1.86(1.16至2.99)(p值 = 0.53)。
女性发生卒中/SE的风险更高,且抗凝治疗使女性卒中/SE事件发生率的降低幅度小于男性。
NCT01090362。