Bassand Jean-Pierre, Accetta Gabriele, Al Mahmeed Wael, Corbalan Ramon, Eikelboom John, Fitzmaurice David A, Fox Keith A A, Gao Haiyan, Goldhaber Samuel Z, Goto Shinya, Haas Sylvia, Kayani Gloria, Pieper Karen, Turpie Alexander G G, van Eickels Martin, Verheugt Freek W A, Kakkar Ajay K
Department of Cardiology-EA 3920, University of Besançon, Besançon, France.
Thrombosis Research Institute, London, United Kingdom.
PLoS One. 2018 Jan 25;13(1):e0191592. doi: 10.1371/journal.pone.0191592. eCollection 2018.
The factors influencing three major outcomes-death, stroke/systemic embolism (SE), and major bleeding-have not been investigated in a large international cohort of unselected patients with newly diagnosed atrial fibrillation (AF).
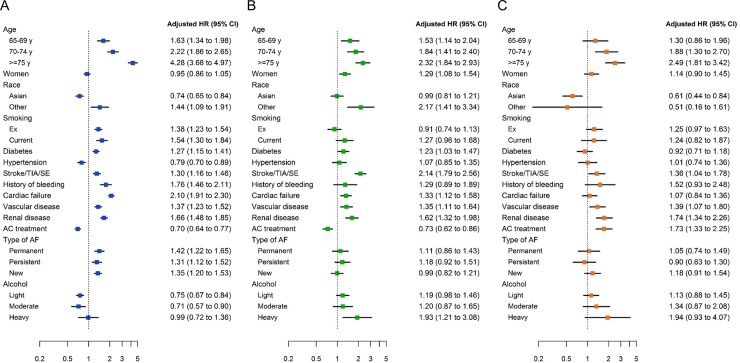
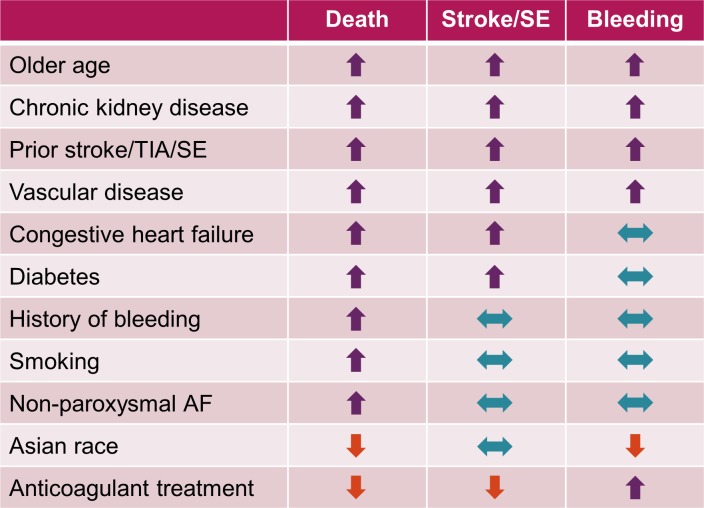
In 28,628 patients prospectively enrolled in the GARFIELD-AF registry with 2-year follow-up, we aimed at analysing: (1) the variables influencing outcomes; (2) the extent of implementation of guideline-recommended therapies in comorbidities that strongly affect outcomes. Median (IQR) age was 71.0 (63.0 to 78.0) years, 44.4% of patients were female, median (IQR) CHA2DS2-VASc score was 3.0 (2.0 to 4.0); 63.3% of patients were on anticoagulants (ACs) with or without antiplatelet (AP) therapy, 24.5% AP monotherapy, and 12.2% no antithrombotic therapy. At 2 years, rates (95% CI) of death, stroke/SE, and major bleeding were 3.84 (3.68; 4.02), 1.27 (1.18; 1.38), and 0.71 (0.64; 0.79) per 100 person-years. Age, history of stroke/SE, vascular disease (VascD), and chronic kidney disease (CKD) were associated with the risks of all three outcomes. Congestive heart failure (CHF) was associated with the risks of death and stroke/SE. Smoking, non-paroxysmal forms of AF, and history of bleeding were associated with the risk of death, female sex and heavy drinking with the risk of stroke/SE. Asian race was associated with lower risks of death and major bleeding versus other races. AC treatment was associated with 30% and 28% lower risks of death and stroke/SE, respectively, compared with no AC treatment. Rates of prescription of guideline-recommended drugs were suboptimal in patients with CHF, VascD, or CKD.
Our data show that several variables are associated with the risk of one or more outcomes, in terms of death, stroke/SE, and major bleeding. Comprehensive management of AF should encompass, besides anticoagulation, improved implementation of guideline-recommended therapies for comorbidities strongly associated with outcomes, namely CHF, VascD, and CKD.
ClinicalTrials.gov NCT01090362.
在一个未经过筛选的新诊断房颤(AF)患者的大型国际队列中,尚未对影响三个主要结局——死亡、卒中/全身性栓塞(SE)和大出血——的因素进行研究。
在28628例前瞻性纳入加菲尔德房颤注册研究并随访2年的患者中,我们旨在分析:(1)影响结局的变量;(2)在对结局有强烈影响的合并症中,指南推荐治疗的实施程度。年龄中位数(四分位间距)为71.0(63.0至78.0)岁,44.4%的患者为女性,CHA2DS2-VASc评分中位数(四分位间距)为3.0(2.0至4.0);63.3%的患者接受抗凝剂(AC)治疗,同时或不同时接受抗血小板(AP)治疗,24.5%的患者接受AP单药治疗,12.2%的患者未接受抗血栓治疗。在2年时,每100人年的死亡、卒中/SE和大出血发生率(95%CI)分别为3.84(3.68;4.02)、1.27(1.18;1.38)和0.71(0.64;0.79)。年龄、卒中/SE病史、血管疾病(VascD)和慢性肾脏病(CKD)与所有这三个结局的风险相关。充血性心力衰竭(CHF)与死亡和卒中/SE的风险相关。吸烟、非阵发性房颤形式和出血史与死亡风险相关,女性和大量饮酒与卒中/SE风险相关。与其他种族相比,亚洲种族的死亡和大出血风险较低。与未接受AC治疗相比,AC治疗分别使死亡和卒中/SE风险降低30%和28%。在CHF、VascD或CKD患者中,指南推荐药物的处方率不理想。
我们的数据表明,就死亡、卒中/SE和大出血而言,有几个变量与一个或多个结局的风险相关。房颤综合管理除抗凝外,还应包括更好地实施针对与结局密切相关的合并症(即CHF、VascD和CKD)的指南推荐治疗。
ClinicalTrials.gov NCT01090362。