Deshmukh Amrish, Kim Gene, Burke Martin, Anyanwu Emeka, Jeevanandam Valluvan, Uriel Nir, Tung Roderick, Ozcan Cevher
Department of Medicine, University of Chicago, IL.
Section of Cardiology, University of Chicago, IL.
J Am Heart Assoc. 2017 Mar 8;6(3):e005340. doi: 10.1161/JAHA.116.005340.
The incidence, predictors, and impact of atrial arrhythmias along with left atrial structural changes in patients with left ventricular assist devices (LVADs) remain undetermined.
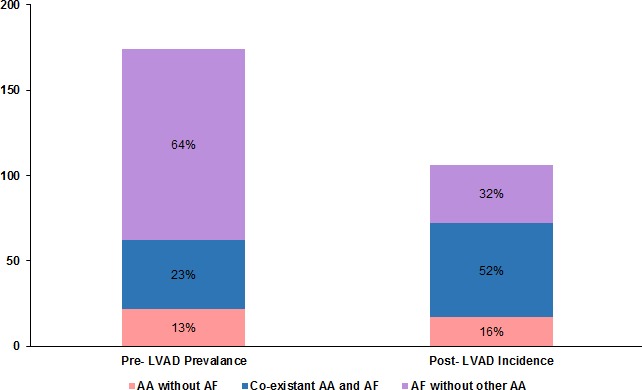
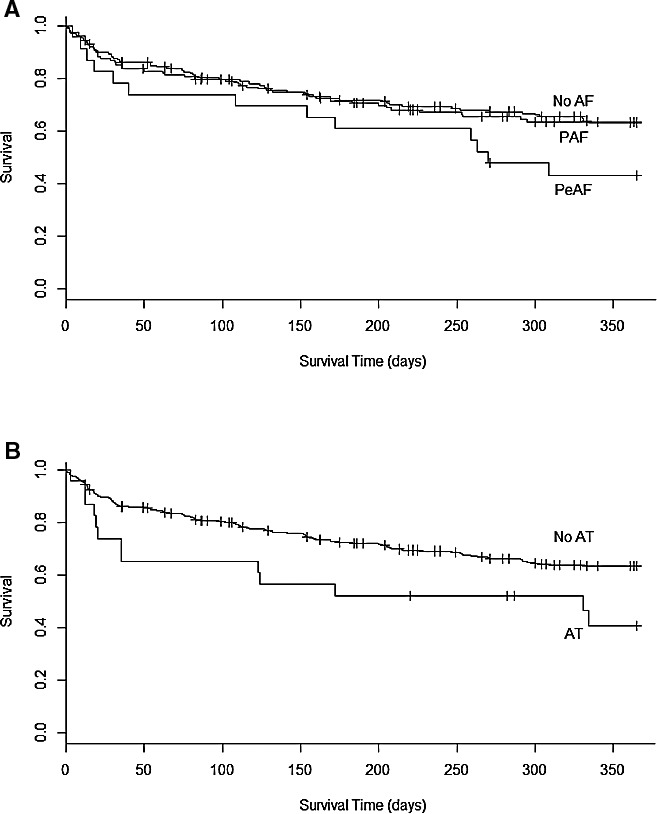
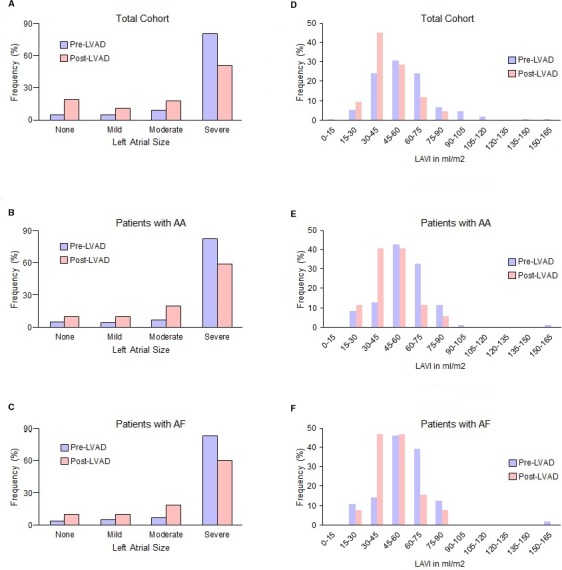
All patients who underwent LVAD implantation from 2008 to 2015 at the University of Chicago Medical Center were included. Electronic medical records, electrocardiograms, echocardiograms, and cardiac electrical device interrogations were reviewed. The association of arrhythmias and clinical covariates with survival was evaluated by Kaplan-Meier and Cox proportional hazards analyses. A total of 331 patients were followed for a median of 330 days (range 0-2306 days). Mean age was 57.8±12.8 years, 256 participants (77.3%) were male, mean left ventricular ejection fraction was 20±6.6%, and 124 (37.5%) had ischemic cardiomyopathy. Atrial arrhythmias (53.8%) were highly prevalent and frequently coexisted before LVAD implantation: atrial fibrillation (AF) in 45.9%, atrial flutter in 13.9%, atrial tachycardia in 6.9%, and atrioventricular nodal reentrant tachycardia in 1.2%. New-onset AF was documented in 14 patients (7.8% of patients without prior AF) after the first 30 days with an LVAD. Increasing age, renal insufficiency, and lung disease were predictors of new-onset AF after LVAD implantation. Of patients with paroxysmal AF, 43% had no further AF after LVAD. Left atrial size and volume index improved with LVAD (<0.005). History of persistent AF, atrial tachycardia, ventricular arrhythmia, coronary artery bypass, and low albumin were associated with decreased survival.
Atrial arrhythmias are significantly prevalent in patients who require LVAD and are associated with increased mortality; however, LVADs induce favorable atrial structural and electrical remodeling.
左心室辅助装置(LVAD)植入患者中心房心律失常的发生率、预测因素及其影响,以及左心房结构变化仍未明确。
纳入2008年至2015年在芝加哥大学医学中心接受LVAD植入的所有患者。回顾电子病历、心电图、超声心动图和心脏电子设备记录。通过Kaplan-Meier和Cox比例风险分析评估心律失常及临床协变量与生存率的相关性。共对331例患者进行了中位时间为330天(范围0 - 2306天)的随访。平均年龄为57.8±12.8岁,256例参与者(77.3%)为男性,平均左心室射血分数为20±6.6%,124例(37.5%)患有缺血性心肌病。心房心律失常(53.8%)非常普遍,且在LVAD植入前常并存:房颤(AF)占45.9%,房扑占13.9%,房性心动过速占6.9%,房室结折返性心动过速占1.2%。LVAD植入后30天内,14例患者(无既往房颤患者的7.8%)记录到新发房颤。年龄增加、肾功能不全和肺部疾病是LVAD植入后新发房颤的预测因素。阵发性房颤患者中,43%在LVAD植入后未再发生房颤。LVAD植入后左心房大小和容积指数有所改善(<0.005)。持续性房颤病史、房性心动过速、室性心律失常、冠状动脉搭桥术和低白蛋白与生存率降低相关。
需要LVAD的患者中心房心律失常显著普遍,且与死亡率增加相关;然而,LVAD可引起有利的心房结构和电重构。