Saleh Mohamed A, Norlander Allison E, Madhur Meena S
Division of Clinical Pharmacology, Department of Medicine, Vanderbilt University Medical Center, Nashville, TN, USA; Department of Pharmacology and Toxicology, Faculty of Pharmacy, Mansoura University, Mansoura, Egypt.
Department of Molecular Physiology and Biophysics, Vanderbilt University, Nashville TN, USA.
JACC Basic Transl Sci. 2016 Dec;1(7):606-616. doi: 10.1016/j.jacbts.2016.07.009. Epub 2016 Nov 16.
To characterize the T cell subsets producing interleukin 17 (IL-17) isoforms A and F in hypertensive kidneys and vessels and determine whether inhibition of IL-17 signaling lowers blood pressure and end-organ damage in a mouse model of hypertension.
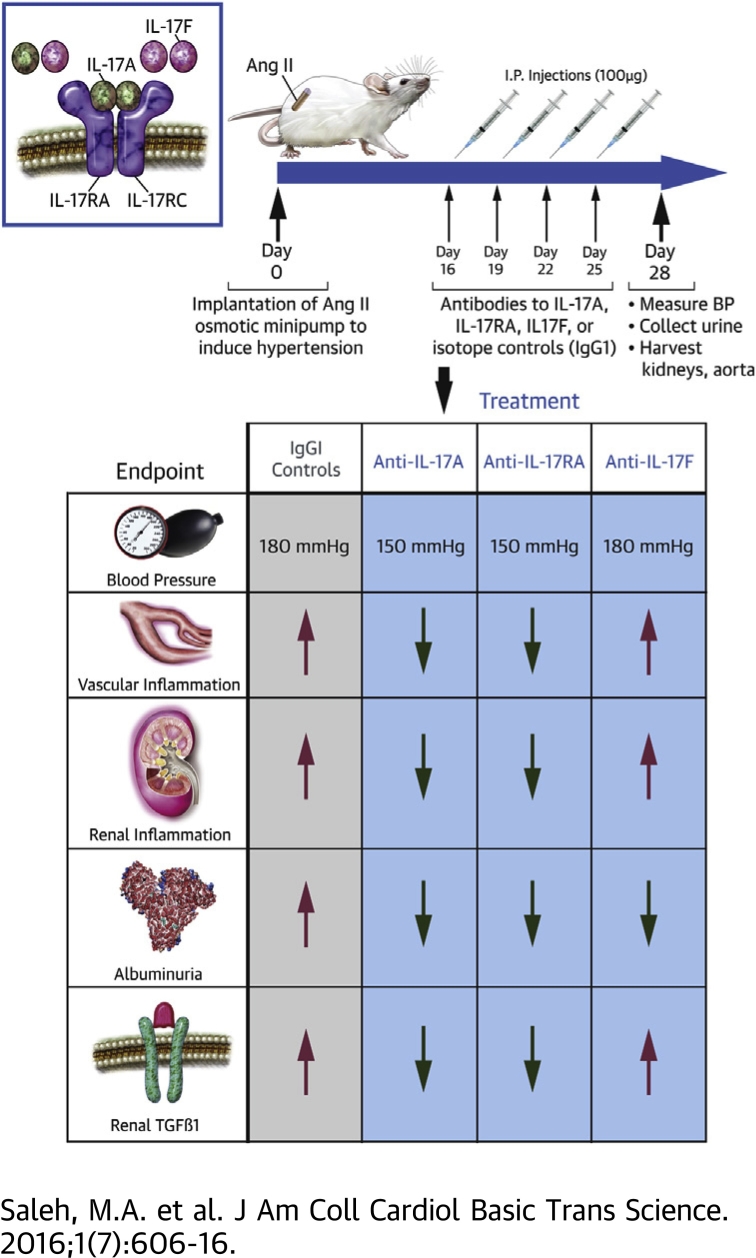
T cell derived cytokines play a central role in the pathophysiology of hypertension and contribute to end-organ dysfunction. We previously showed that mice genetically deficient in IL-17A exhibited blunted hypertension and reduced renal and vascular dysfunction in response to angiotensin II (Ang II) infusion. Monoclonal antibodies to IL-17 isoforms or the IL-17 receptor are emerging as novel therapeutics for psoriasis and related autoimmune disorders.
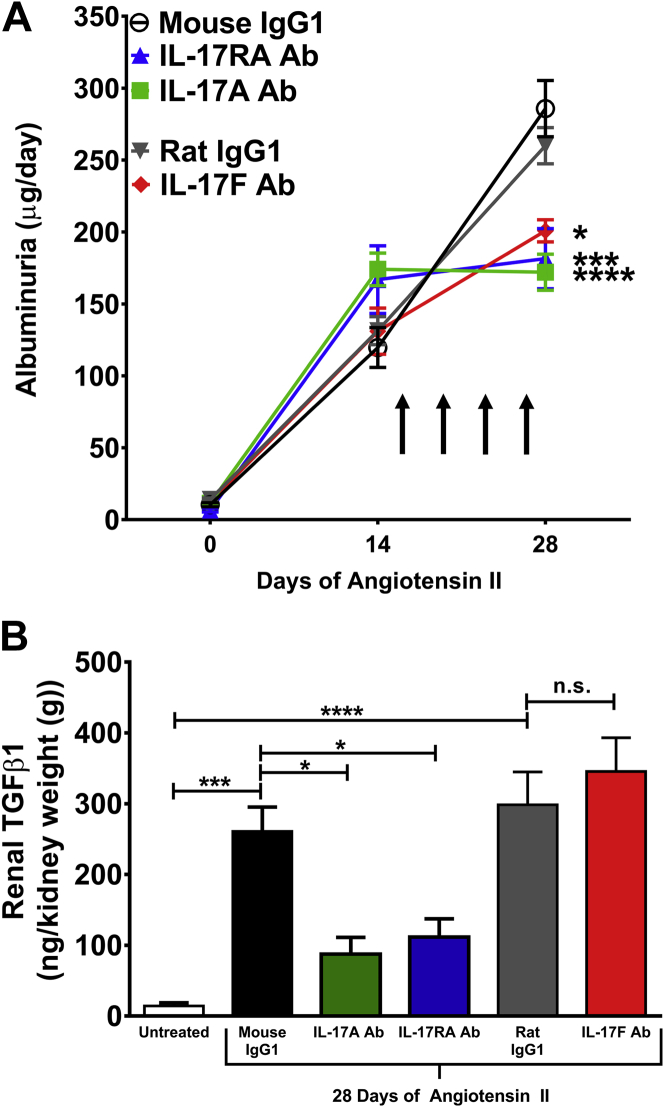
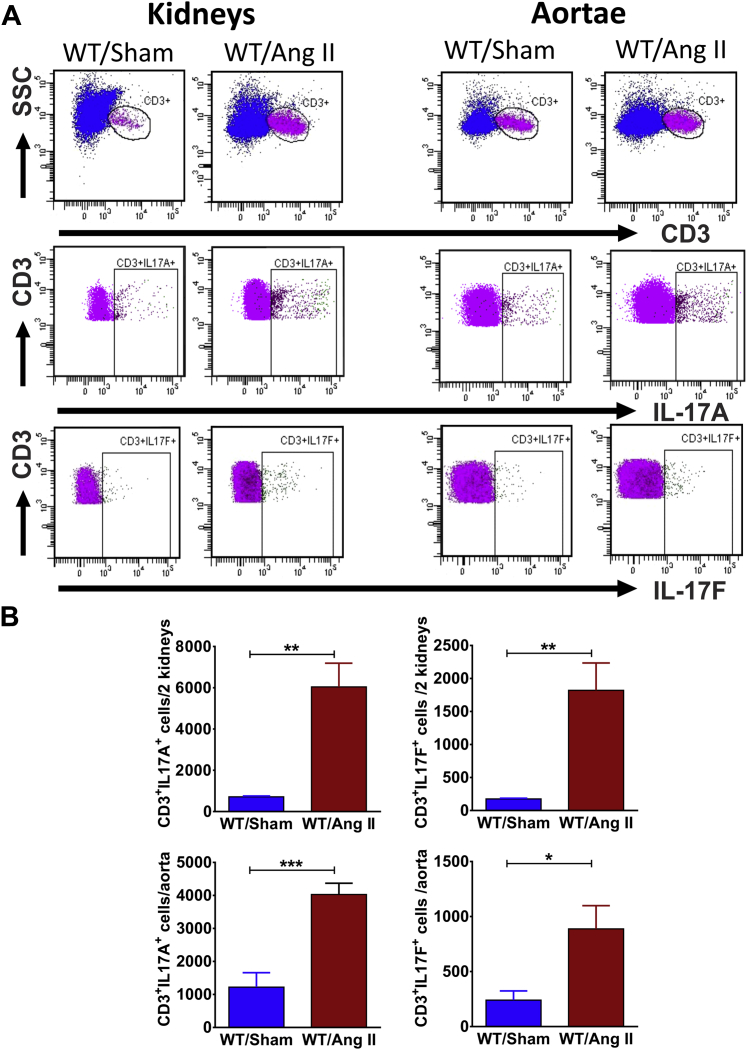
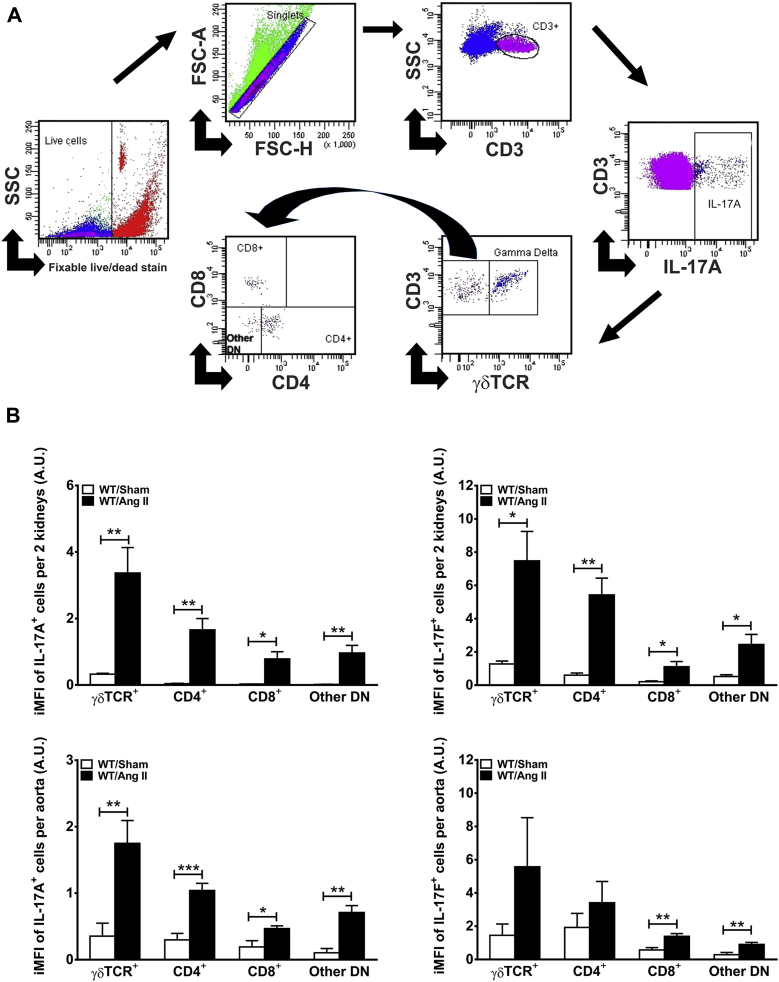
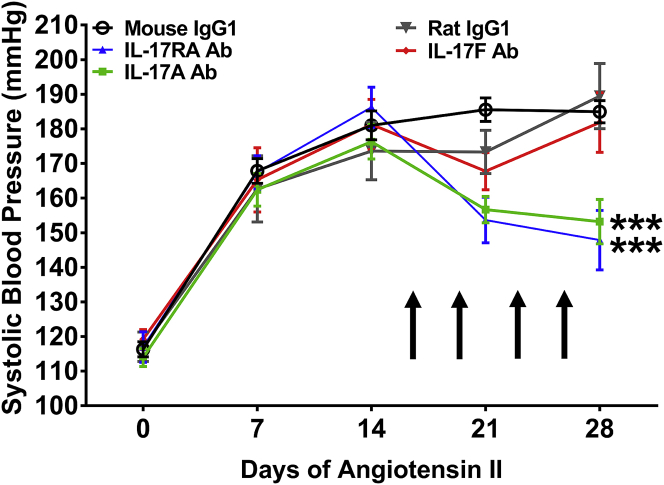
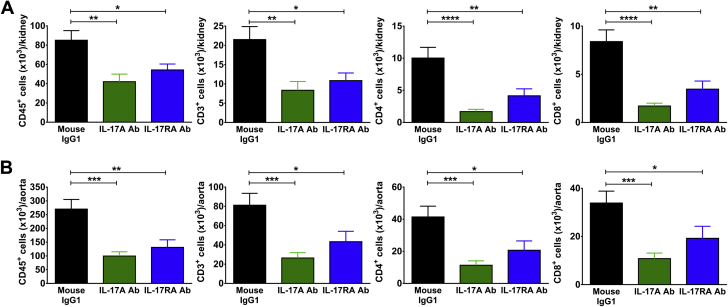
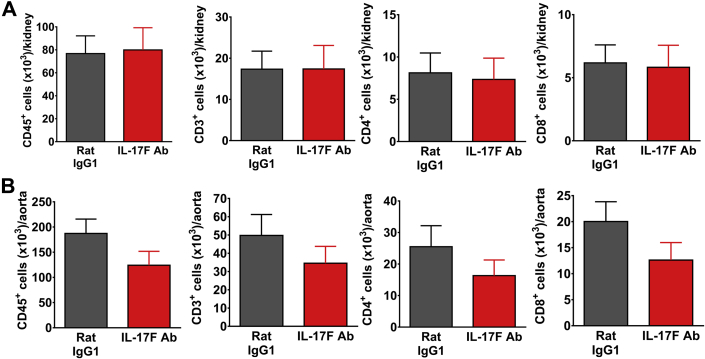
Mice were infused with Ang II for 4 weeks to induce hypertension. Using flow cytometry and intracellular staining, we determined that the primary T cell subsets producing IL-17A and IL-17F in the kidney and aorta are gamma delta (γδ) T cells and CD4+ T helper 17 (T17) cells. Monoclonal antibodies were administered twice weekly starting 2 weeks after the onset of Ang II infusion. Antibodies to IL-17A or the IL-17 receptor A subunit (IL-17RA), but not IL-17F, lowered blood pressure by 30 mmHg, attenuated renal and vascular lymphocyte infiltration, and reduced renal transforming growth factor beta (TGFβ) levels (a marker of renal fibrosis) compared to control IgG1 antibodies. Inhibition of IL-17 signaling also blunted the progression of albuminuria.
Monoclonal antibodies to IL-17A or IL-17RA, but not IL-17F, may be a useful adjunct treatment for hypertension and the associated end-organ dysfunction.
鉴定高血压肾脏和血管中产生白细胞介素17(IL-17)A和F亚型的T细胞亚群,并确定在高血压小鼠模型中抑制IL-17信号传导是否能降低血压和减轻靶器官损伤。
T细胞衍生的细胞因子在高血压的病理生理学中起核心作用,并导致靶器官功能障碍。我们之前表明,IL-17A基因缺陷的小鼠在输注血管紧张素II(Ang II)时表现出血压升高减弱以及肾脏和血管功能障碍减轻。抗IL-17亚型或IL-17受体的单克隆抗体正在成为治疗银屑病和相关自身免疫性疾病的新型疗法。
给小鼠输注Ang II 4周以诱导高血压。使用流式细胞术和细胞内染色,我们确定肾脏和主动脉中产生IL-17A和IL-17F的主要T细胞亚群是γδ T细胞和CD4 +辅助性T细胞17(T17)细胞。从Ang II输注开始2周后,每周两次给予单克隆抗体。与对照IgG1抗体相比,抗IL-17A或IL-17受体A亚基(IL-17RA)的抗体,但不是抗IL-17F的抗体,可使血压降低30 mmHg,减轻肾脏和血管淋巴细胞浸润,并降低肾脏转化生长因子β(TGFβ)水平(肾脏纤维化的标志物)。抑制IL-17信号传导也减弱了蛋白尿的进展。
抗IL-17A或IL-17RA的单克隆抗体,而非抗IL-17F的单克隆抗体,可能是高血压及相关靶器官功能障碍的有用辅助治疗方法。