Schwab T R, Stillhard P F, Schibli S, Furrer M, Sommer C
Kantonsspital Graubünden, Loestrasse 170, 7000, Chur, Switzerland.
Eur J Trauma Emerg Surg. 2018 Apr;44(2):235-243. doi: 10.1007/s00068-017-0775-9. Epub 2017 Mar 9.
The incidence of radial nerve injury after humeral shaft fractures is on average 11.8% (Shao et al., J Bone Jt Surg Br 87(12):1647-1652, 2005) representing the most common peripheral nerve injury associated with long bone fractures (Korompilias et al., Injury, 2013). The purpose of this study was to analyze our current policy and long-term outcome, regarding surgically treated humeral shaft fractures in combination with radial nerve palsy.
We retrospectively analyzed the data of patients with surgically treated humeral shaft fractures from 01/01/2003 to 28/02/2013. The analysis included fracture type, soft tissue injury regarding closed and open fractures, type of fixation, management, and outcome of radial nerve palsy.
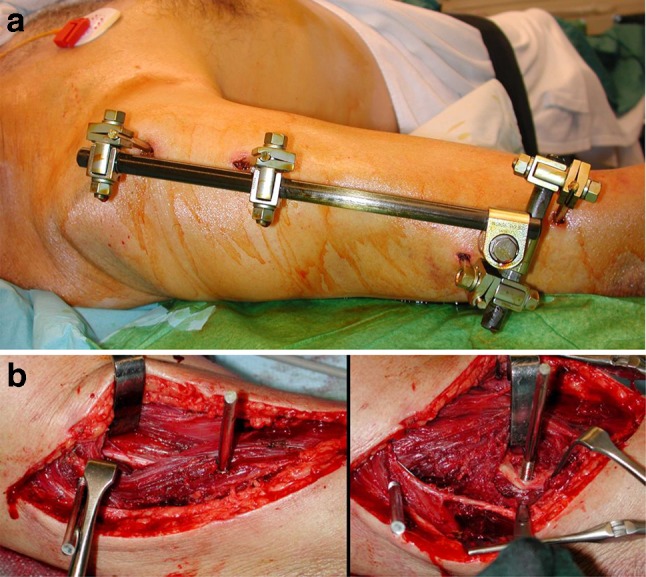
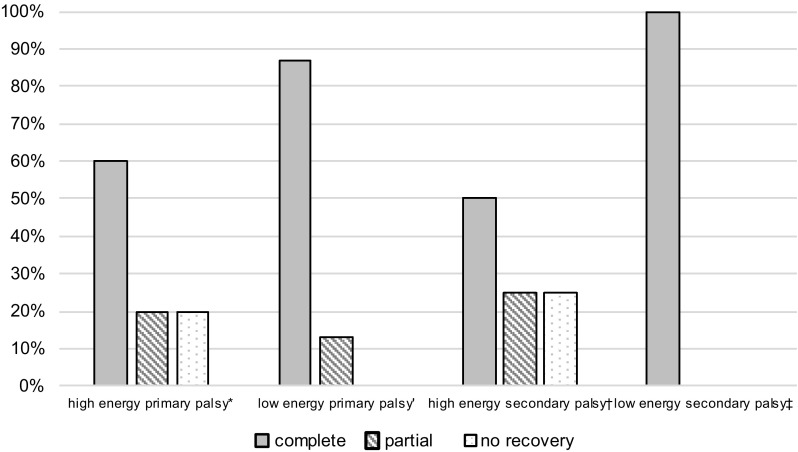
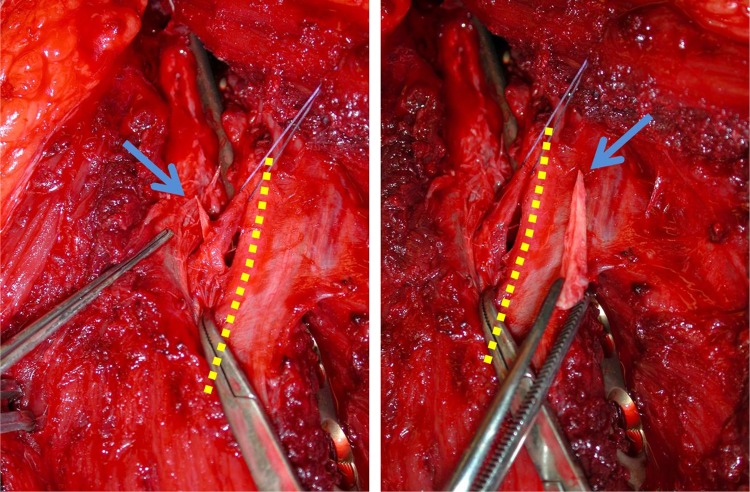
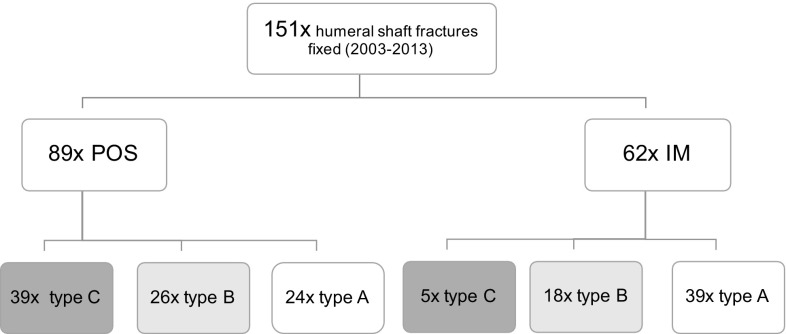
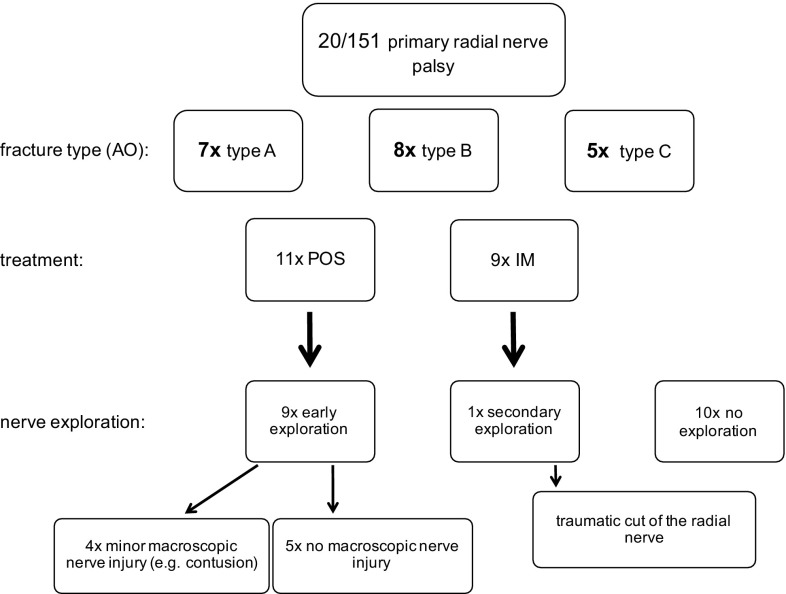
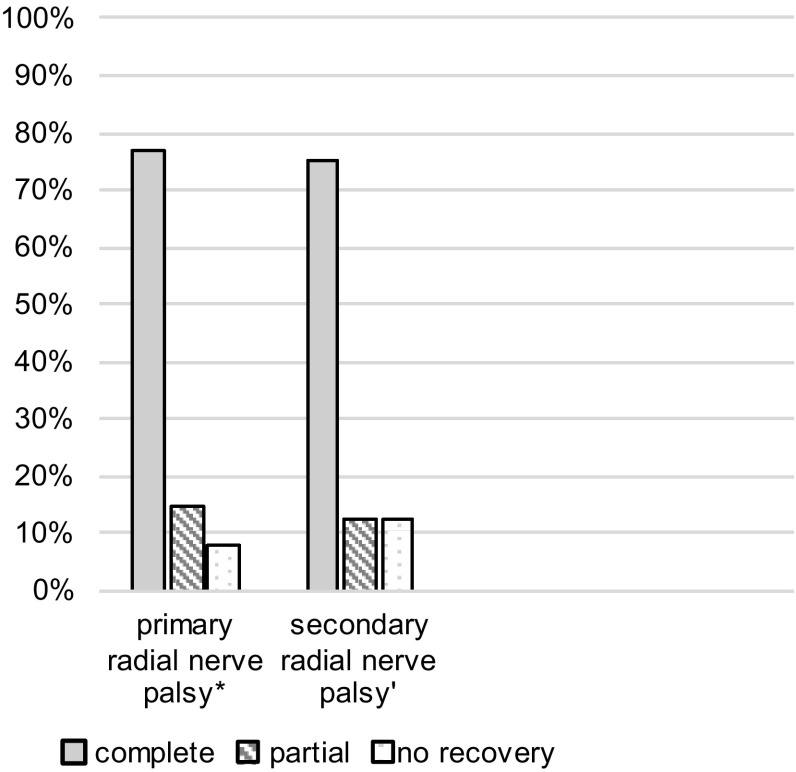
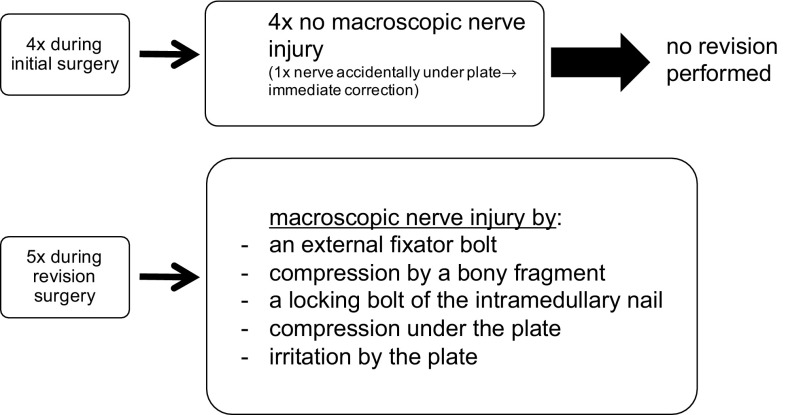
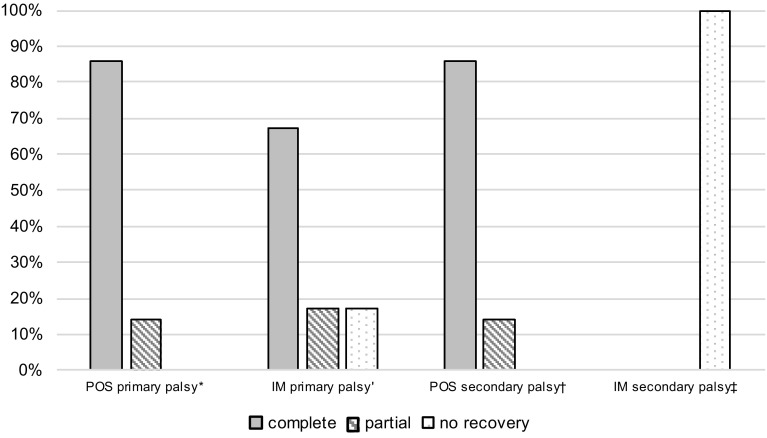
A total of 151 humeral shaft fractures were fixed in our hospital. In 20 (13%) cases, primary radial palsy was observed. Primary nerve exploration was performed in nine cases. Out of the 13 patients with follow-up, 10 showed a complete, 2 a partial, and 1 a minimal nerve recovery. Two of them underwent a revision procedure. Secondary radial nerve palsy occurred in 9 (6%) patients postoperatively. In five patients, the radial nerve was not exposed during the initial surgery and, therefore, underwent revision with nerve exploration. In all 5, a potential cause for the palsy was found and corrected as far as possible with full recovery in 3 and minimal recovery in one patient. In four patients with exposure of the nerve during the initial surgery, no revision was performed. All of these 4 showed a full recovery.
Our study showed an overall rate of 19% radial nerve palsy in surgically treated humeral shaft fractures. Most of the primary palsies (13%) recovered spontaneously, and therefore, nerve exploration was only exceptionally needed. The incidence of secondary palsy after surgery (6%) was high and mainly seen after plate fixation. In these cases, we recommend early nerve exploration, to detect and treat potential curable neural lesions.
肱骨干骨折后桡神经损伤的发生率平均为11.8%(Shao等人,《骨与关节外科杂志(英国)》87(12):1647 - 1652, 2005),是长骨骨折相关的最常见周围神经损伤(Korompilias等人,《损伤》,2013)。本研究的目的是分析我们目前对于手术治疗肱骨干骨折合并桡神经麻痹的策略及长期疗效。
我们回顾性分析了2003年1月1日至2013年2月28日期间接受手术治疗的肱骨干骨折患者的数据。分析内容包括骨折类型、闭合性和开放性骨折的软组织损伤情况、固定类型、处理方式以及桡神经麻痹的结局。
我院共固定了151例肱骨干骨折。其中20例(13%)出现原发性桡神经麻痹。9例进行了一期神经探查。在13例接受随访的患者中,10例完全恢复,2例部分恢复,1例轻微恢复。其中2例接受了翻修手术。9例(6%)患者术后出现继发性桡神经麻痹。5例患者在初次手术时未暴露桡神经,因此接受了神经探查翻修手术。在所有这5例患者中,均发现了麻痹的潜在原因并尽可能进行了纠正,3例完全恢复,1例轻微恢复。在初次手术时神经已暴露的4例患者中,未进行翻修手术。这4例患者均完全恢复。
我们的研究表明,手术治疗的肱骨干骨折中桡神经麻痹的总体发生率为19%。大多数原发性麻痹(13%)可自发恢复,因此仅在极少数情况下需要进行神经探查。术后继发性麻痹的发生率(6%)较高,主要见于钢板固定后。在这些病例中,我们建议早期进行神经探查,以发现并治疗潜在的可治愈神经损伤。