Pajnigara Natasha, Kolte Abhay, Kolte Rajashri, Pajnigara Nilufer, Lathiya Vrushali
Department of Periodontics and Implantology, VSPM Dental College and Research Centre, Nagpur, Maharashtra, India.
Department of Oral Medicine and Radiology, VSPM Dental College and Research Centre, Nagpur, Maharashtra, India.
J Indian Soc Periodontol. 2016 Jul-Aug;20(4):386-390. doi: 10.4103/0972-124X.192307.
Decision-making in periodontal therapeutics is critical and is influenced by accurate diagnosis of osseous defects, especially furcation involvement. Commonly used diagnostic methods such as clinical probing and conventional radiography have their own limitations. Hence, this study was planned to evaluate the dimensions of furcation defects clinically (pre- and post-surgery), intra-surgically, and by cone beam computed tomography (CBCT) (pre- and post-surgery).
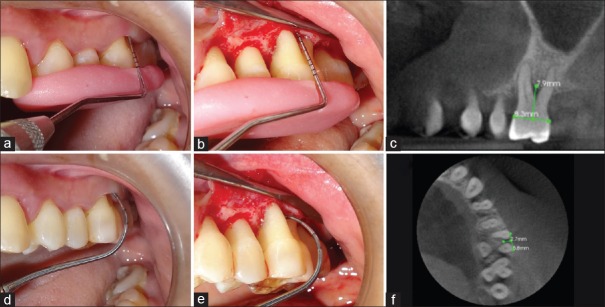
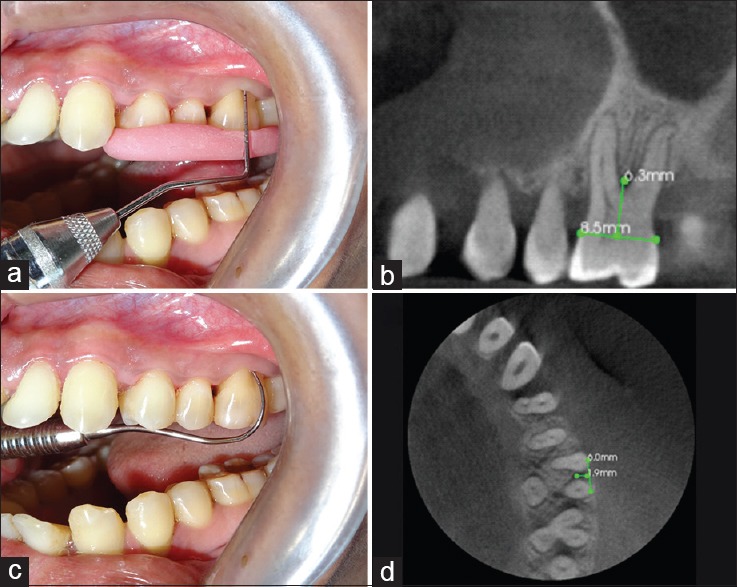
The study comprised a total of 200 Grade II furcation defects in forty patients, with a mean age of 38.05 ± 4.77 years diagnosed with chronic periodontitis which were evaluated clinically (pre- and post-surgically), by CBCT (pre- and post-surgically), and intrasurgically after flap reflection (40 defects in each). After the presurgical clinical and CBCT measurements, demineralized freeze-dried bone allograft was placed in the furcation defect and the flaps were sutured back. Six months later, these defects were evaluated by recording measurements clinically, i.e., postsurgery clinical measurements and also postsurgery CBCT measurements (40 defects each).
Presurgery clinical measurements (vertical 6.15 ± 1.71 mm and horizontal 3.05 ± 0.84 mm) and CBCT measurements (vertical 7.69 ± 1.67 mm and horizontal 4.62 ± 0.77 mm) underestimated intrasurgery measurements (vertical 8.025 ± 1.67 mm and horizontal 4.82 ± 0.67 mm) in both vertical and horizontal aspects, and the difference was statistically not significant (vertical = 1.000, 95% confidence interval [CI], horizontal = 0.867, 95% CI). Further, postsurgery clinical measurements (vertical 2.9 ± 0.74 mm and horizontal 1.52 ± 0.59 mm) underestimated CBCT measurements (vertical 3.67 ± 1.17 mm and horizontal 2.45 ± 0.48 mm). There was statistically significant difference between presurgery clinical-presurgery CBCT ( < 0.0001, 95% CI) versus postsurgery clinical-postsurgery CBCT ( < 0.0001, 95% CI) values in both vertical and horizontal aspects.
The use of CBCT appears to be prudent for accurate diagnosis of furcation defects in advanced periodontal diseases. Presurgical and postsurgical three-dimensional imaging enable the clinician to optimize treatment decisions and assess the quantum of healing more definitively.
牙周治疗中的决策至关重要,且受到骨缺损尤其是根分叉病变准确诊断的影响。常用的诊断方法如临床探诊和传统放射成像都有其局限性。因此,本研究旨在通过临床(手术前后)、术中及锥形束计算机断层扫描(CBCT)(手术前后)评估根分叉病变的尺寸。
本研究共纳入40例患者的200处II度根分叉病变,患者平均年龄为38.05±4.77岁,均诊断为慢性牙周炎,分别通过临床(手术前后)、CBCT(手术前后)及翻瓣术后术中(各40处病变)进行评估。术前临床及CBCT测量后,将脱矿冻干骨移植体置于根分叉病变处,然后将瓣复位缝合。6个月后,通过记录临床测量值(即术后临床测量值)及术后CBCT测量值(各40处病变)对这些病变进行评估。
术前临床测量值(垂直方向6.15±1.71mm,水平方向3.05±0.84mm)及CBCT测量值(垂直方向