Jowhari Fahd, Hopman Wilma M, Hookey Lawrence
Gastrointestinal Diseases Research Unit, Kingston General Hospital, Queen's University, Kingston, Ontario, Canada.
Clinical Research Centre, Kingston General Hospital, and Department of Public Health Sciences, Queen's University, Kingston, Ontario, Canada.
Endosc Int Open. 2017 Mar;5(3):E172-E178. doi: 10.1055/s-0043-102934.
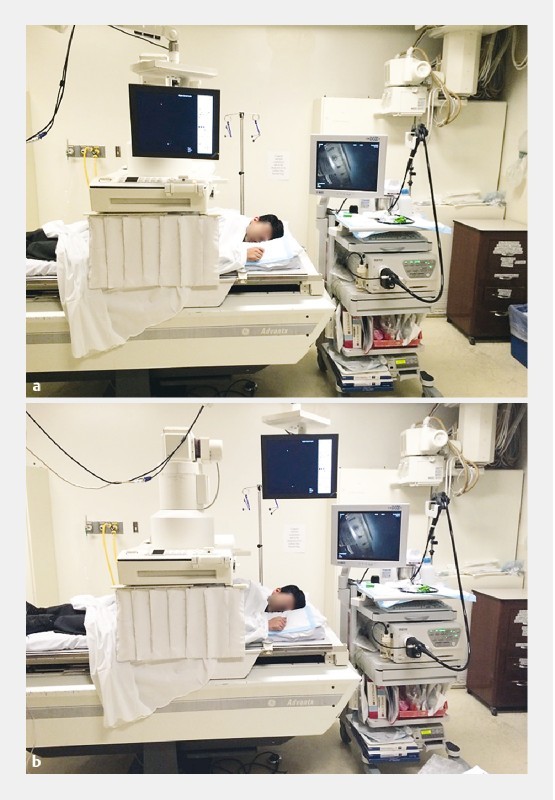
Endoscopic retrograde cholangiopancreatgraphy (ERCP) carries a radiation risk to patients undergoing the procedure and the team performing it. Fluoroscopy time (FT) has been shown to have a linear relationship with radiation exposure during ERCP. Recent modifications to our ERCP suite design were felt to impact fluoroscopy time and ergonomics. This multivariate analysis was therefore undertaken to investigate these effects, and to identify and validate various clinical, procedural and ergonomic factors influencing the total fluoroscopy time during ERCP. This would better assist clinicians with predicting prolonged fluoroscopic durations and to undertake relevant precautions accordingly. A retrospective analysis of 299 ERCPs performed by 4 endoscopists over an 18-month period, at a single tertiary care center was conducted. All inpatients/outpatients (121 males, 178 females) undergoing ERCP for any clinical indication from January 2012 to June 2013 in the chosen ERCP suite were included in the study. Various predetermined clinical, procedural and ergonomic factors were obtained via chart review. Univariate analyses identified factors to be included in the multivariate regression model with FT as the dependent variable. Bringing the endoscopy and fluoroscopy screens next to each other was associated with a significantly lesser FT than when the screens were separated further (-1.4 min, = 0.026). Other significant factors associated with a prolonged FT included having a prior ERCP (+ 1.4 min, = 0.031), and more difficult procedures (+ 4.2 min for each level of difficulty, < 0.001). ERCPs performed by high-volume endoscopists used lesser FT vs. low-volume endoscopists (-1.82, P = 0.015). Our study has identified and validated various factors that affect the total fluoroscopy time during ERCP. This is the first study to show that decreasing the distance between the endoscopy and fluoroscopy screens in the ERCP suite significantly reduces the total fluoroscopy time, and therefore radiation exposure to patients and staff involved in the procedure.
内镜逆行胰胆管造影术(ERCP)会给接受该手术的患者及实施手术的团队带来辐射风险。透视时间(FT)已被证明与ERCP期间的辐射暴露呈线性关系。我们对ERCP手术室设计的近期改进被认为会影响透视时间和人体工程学。因此,进行了这项多变量分析,以研究这些影响,并识别和验证影响ERCP期间总透视时间的各种临床、手术和人体工程学因素。这将更好地帮助临床医生预测延长的透视持续时间,并相应地采取相关预防措施。对一家三级医疗中心的4位内镜医师在18个月内进行的299例ERCP手术进行了回顾性分析。2012年1月至2013年6月在选定的ERCP手术室因任何临床指征接受ERCP的所有住院/门诊患者(121名男性,178名女性)均纳入研究。通过病历审查获得各种预先确定的临床、手术和人体工程学因素。单变量分析确定了以FT为因变量纳入多变量回归模型的因素。将内镜和透视屏幕彼此靠近放置时的FT显著低于屏幕分隔更远时(-1.4分钟,P = 0.026)。与延长FT相关的其他显著因素包括既往有ERCP手术史(+1.4分钟,P = 0.031),以及手术难度更大(每增加一个难度级别增加+4.2分钟,P < 0.001)。高年资内镜医师进行的ERCP手术的FT低于低年资内镜医师(-1.82,P = 0.015)。我们的研究识别并验证了影响ERCP期间总透视时间的各种因素。这是第一项表明在ERCP手术室中缩短内镜和透视屏幕之间的距离可显著减少总透视时间,从而减少参与手术的患者和工作人员所受辐射暴露的研究