Siow Sze Li, Mahendran Hans Alexander, Wong Chee Ming, Milaksh Nirumal Kumar, Nyunt Myo
Department of Surgery, Faculty of Medicine and Health Sciences, Universiti Malaysia Sarawak, 94300, Kota Samarahan, Kuching, Sarawak, Malaysia.
Department of Surgery, Jalan Hospital, 93586, Kuching, Sarawak, Malaysia.
BMC Surg. 2017 Mar 20;17(1):25. doi: 10.1186/s12893-017-0221-2.
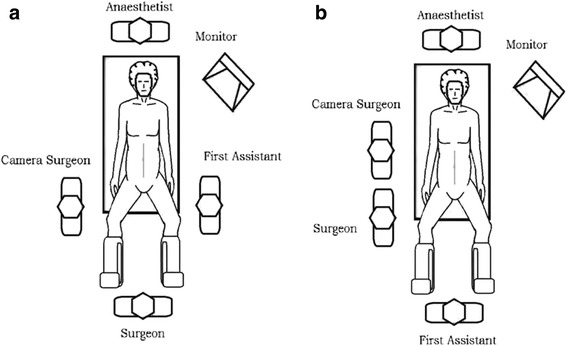
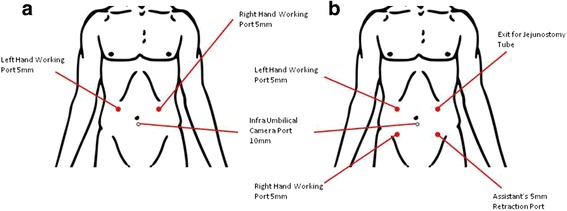
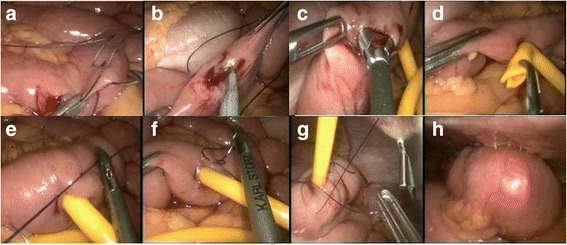
In recent years, staging laparoscopy has gained acceptance as part of the assessment of resectability of upper gastrointestinal (UGI) malignancies. Not infrequently, we encounter tumours that are either locally advanced; requiring neoadjuvant therapy or occult peritoneal disease that requires palliation. In all these cases, the establishment of enteral feeding during staging laparoscopy is important for patients' nutrition. This review describes our technique of performing laparoscopic feeding jejunostomy and the clinical outcomes.
The medical records of all patients who underwent laparoscopic feeding jejunostomy following staging laparoscopy for UGI malignancies between January 2010 and July 2015 were retrospectively reviewed. The data included patient demographics, operative technique and clinical outcomes.
Fifteen patients (11 males) had feeding jejunostomy done when staging laparoscopy showed unresectable UGI maligancy. Eight (53.3%) had gastric carcinoma, four (26.7%) had oesophageal carcinoma and three (20%) had cardio-oesophageal junction carcinoma. The mean age was 63.3 ± 7.3 years. Mean operative time was 66.0 ± 7.4 min. Mean postoperative stay was 5.6 ± 2.2 days. Laparoscopic feeding jejunostomy was performed without intra-operative complications. There were no major complications requiring reoperation but four patients had excoriation at the T-tube site and three patients had tube dislodgement which required bedside replacement of the feeding tube. The mean duration of feeding tube was 127.3 ± 99.6 days.
Laparoscopic feeding jejunostomy is an important adjunct to staging laparoscopy that can be performed safely with low morbidity. Meticulous attention to surgical techniques is the cornerstone of success.
近年来,分期腹腔镜检查已被认可为评估上消化道(UGI)恶性肿瘤可切除性的一部分。我们经常遇到局部进展期肿瘤,需要新辅助治疗,或者遇到隐匿性腹膜疾病需要姑息治疗。在所有这些情况下,在分期腹腔镜检查期间建立肠内营养对患者的营养状况很重要。本综述描述了我们进行腹腔镜下空肠造口术的技术及临床结果。
回顾性分析2010年1月至2015年7月期间因UGI恶性肿瘤接受分期腹腔镜检查后行腹腔镜下空肠造口术的所有患者的病历。数据包括患者人口统计学资料、手术技术和临床结果。
15例患者(11例男性)在分期腹腔镜检查显示UGI恶性肿瘤不可切除时行空肠造口术。8例(53.3%)为胃癌,4例(26.7%)为食管癌,3例(20%)为贲门癌。平均年龄为63.3±7.3岁。平均手术时间为66.0±7.4分钟。平均术后住院时间为5.6±2.2天。腹腔镜下空肠造口术无术中并发症。无需要再次手术的重大并发症,但4例患者T管部位有皮肤擦伤,3例患者出现导管移位,需要在床边更换饲管。饲管平均留置时间为127.3±99.6天。
腹腔镜下空肠造口术是分期腹腔镜检查的重要辅助手段,可安全进行,发病率低。对手术技术的细致关注是成功的基石。