Maziarz Marlena, Kinyera Tobias, Otim Isaac, Kagwa Paul, Nabalende Hadijah, Legason Ismail D, Ogwang Martin D, Kirimunda Samuel, Emmanuel Benjamin, Reynolds Steven J, Kerchan Patrick, Joloba Moses M, Bergen Andrew W, Bhatia Kishor, Talisuna Ambrose O, Biggar Robert J, Goedert James J, Pfeiffer Ruth M, Mbulaiteye Sam M
Division of Cancer Epidemiology and Genetics, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA.
EMBLEM Study, African Field Epidemiology Network, Kampala, Uganda.
Malar J. 2017 Mar 20;16(1):124. doi: 10.1186/s12936-017-1778-z.
Falciparum malaria is an important risk factor for African Burkitt lymphoma (BL), but few studies have evaluated malaria patterns in healthy BL-age children in populations where both diseases are endemic. To obtain accurate current data, patterns of asymptomatic malaria were investigated in northern Uganda, where BL is endemic.
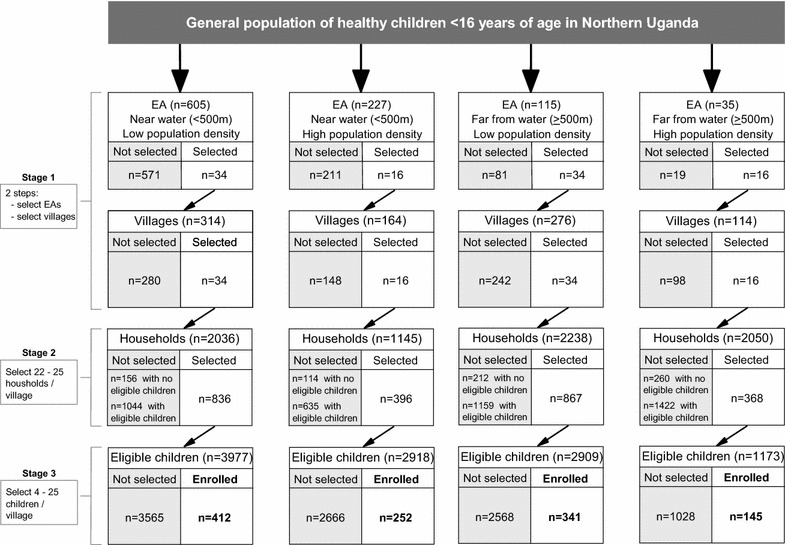
Between 2011 and 2015, 1150 apparently healthy children under 15 years old were sampled from 100 villages in northern Uganda using a stratified, multi-stage, cluster survey design. Falciparum malaria prevalence (pfPR) was assessed by questionnaire, rapid diagnostic test (RDT) and thick film microscopy (TFM). Weighted pfPR and unadjusted and adjusted associations of prevalence with covariates were calculated using logistic models and survey methods.
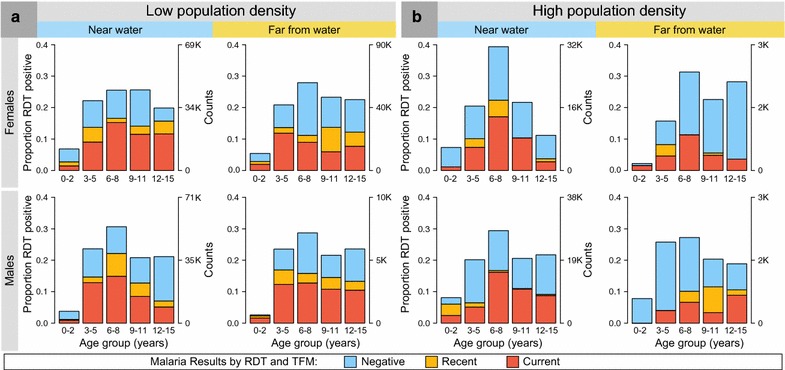
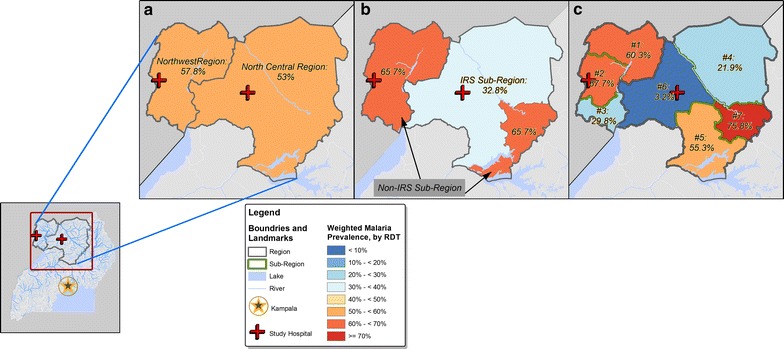
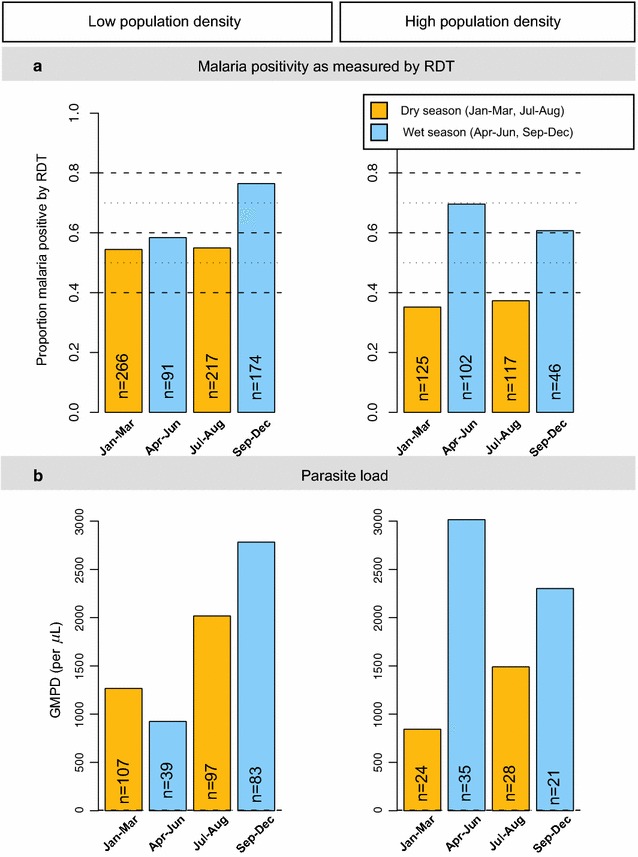
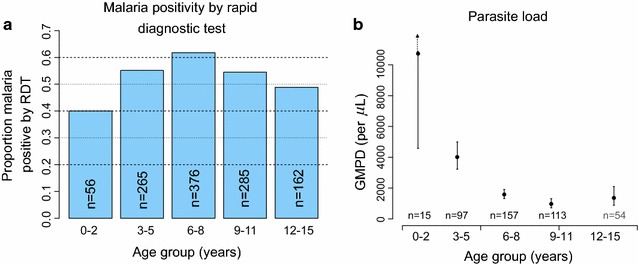
Based on 1143 children successfully tested, weighted pfPR was 54.8% by RDT and 43.4% by TFM. RDT sensitivity and specificity were 97.5 and 77.8%, respectively, as compared to TFM, because RDT detect malaria antigens, which persist in peripheral blood after clinical malaria, thus results based on RDT are reported. Weighted pfPR increased from 40% in children aged under 2 years to 61.8% in children aged 6-8 years (odds ratio 2.42, 95% confidence interval (CI) 1.26-4.65), then fell slightly to 49% in those aged 12-15 years. Geometric mean parasite density was 1805.5 parasites/µL (95% CI 1344.6-2424.3) among TFM-positive participants, and it was higher in children aged <5 years at 5092.9/µL (95% CI 2892.7-8966.8) and lower in those aged ≥10 years at 983.8/µL (95% CI 472.7-2047.4; P = 0.001). Weighted pfPR was lower in children residing in sub-regions employing indoor residual spraying (IRS) than in those residing in non-IRS sub-regions (32.8 versus 65.7%; OR 0.26, 95% CI 0.14, 0.46). However, pfPR varied both within IRS (3.2-55.3%) and non-IRS sub-regions (29.8-75.8%; Pheterogeneity <0.001). pfPR was inversely correlated with a child's mother's income (P = 0.011) and positively correlated with being enrolled in the wet season (P = 0.076), but sex was irrelevant.
The study observed high but geographically and demographically heterogenous patterns of asymptomatic malaria prevalence among children living in northern Uganda. These results provide important baseline data that will enable precise evaluation of associations between malaria and BL.
恶性疟是非洲伯基特淋巴瘤(BL)的一个重要危险因素,但在这两种疾病均为地方病的人群中,很少有研究评估健康的BL发病年龄儿童的疟疾感染模式。为获取准确的当前数据,在BL为地方病的乌干达北部地区对无症状疟疾感染模式进行了调查。
2011年至2015年期间,采用分层、多阶段整群抽样调查设计,从乌干达北部100个村庄抽取了1150名15岁以下看似健康的儿童。通过问卷调查、快速诊断检测(RDT)和厚血膜显微镜检查(TFM)评估恶性疟患病率(pfPR)。使用逻辑模型和调查方法计算加权pfPR以及患病率与协变量的未调整和调整后的关联。
基于1143名成功检测的儿童,RDT检测的加权pfPR为54.8%,TFM检测的为43.4%。与TFM相比,RDT的敏感性和特异性分别为97.5%和77.8%,因为RDT检测疟原虫抗原,这些抗原在临床疟疾发作后仍会在外周血中持续存在,因此报告基于RDT的结果。加权pfPR从2岁以下儿童的40%增至6 - 8岁儿童的61.8%(比值比2.42,95%置信区间(CI)1.26 - 4.65),然后在12 - 15岁儿童中略有下降至49%。TFM检测呈阳性的参与者中,几何平均寄生虫密度为1805.5个寄生虫/微升(95% CI 1344.6 - 2424.3),5岁以下儿童中更高,为5092.9/微升(95% CI 2892.7 - 8966.8),10岁及以上儿童中较低,为983.8/微升(95% CI 472.7 - 2047.4;P = 0.001)。采用室内滞留喷洒(IRS)的次区域儿童的加权pfPR低于未采用IRS的次区域儿童(32.8%对65.7%;OR 0.26,95% CI 0.14,0.46)。然而,pfPR在采用IRS的次区域(3.2% - 55.3%)和未采用IRS的次区域(29.8% - 75.8%)内均有变化(异质性P < 0.001)。pfPR与儿童母亲的收入呈负相关(P = 0.011),与在雨季登记呈正相关(P = 0.076),但与性别无关。
该研究观察到乌干达北部儿童中无症状疟疾患病率较高,但在地理和人口统计学上存在异质性模式。这些结果提供了重要的基线数据,将有助于精确评估疟疾与BL之间的关联。