Ogimi Chikara, Waghmare Alpana A, Kuypers Jane M, Xie Hu, Yeung Cecilia C, Leisenring Wendy M, Seo Sachiko, Choi Su-Mi, Jerome Keith R, Englund Janet A, Boeckh Michael
Vaccine and Infectious Disease Division, Fred Hutchinson Cancer Research Center.
Department of Pediatrics, University of Washington.
Clin Infect Dis. 2017 Jun 1;64(11):1532-1539. doi: 10.1093/cid/cix160.
BACKGROUND.: The possible role of human coronavirus (HCoV) in lower respiratory tract disease (LRTD) in hematopoietic cell transplant (HCT) recipients and patients with hematologic malignancies (HM) has not been well studied.
METHODS.: We conducted a retrospective review of HCT/HM patients with HCoV detected in bronchoalveolar lavage (BAL). HCoV strains were identified in BAL samples using strain-specific polymerase chain reaction. Mortality rates were compared among HCT recipients with LRTD caused by HCoV, respiratory syncytial virus (RSV), influenza virus, or parainfluenza virus (PIV) by multivariable Cox regression analysis.
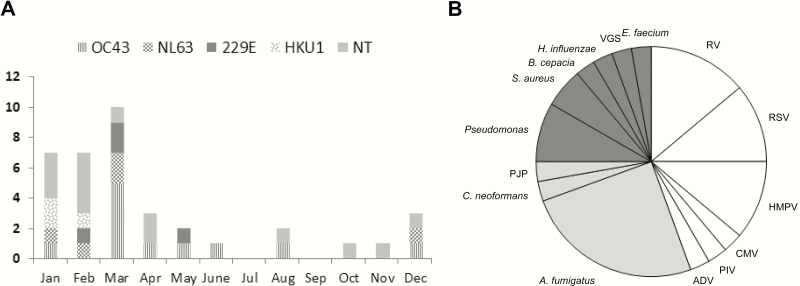
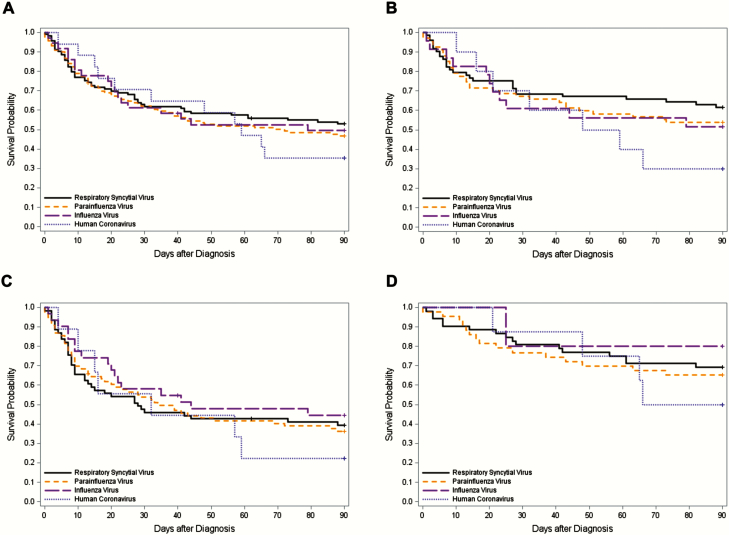
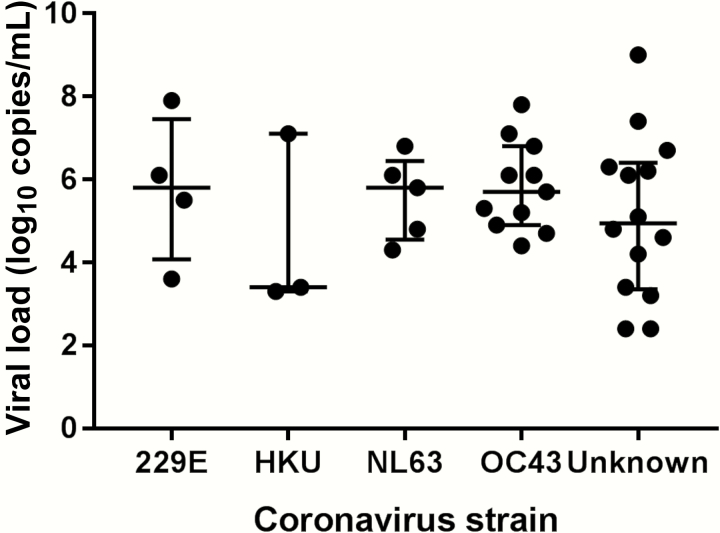
RESULTS.: We identified 35 patients (37 episodes) with HCoV LRTD. Among 23 available BAL samples, 48% were strain OC43, 22% were NL63, 17% were 229E, and 13% were HKU1. Overall, 21 patients (60%) required oxygen therapy at diagnosis and 19 (54%) died within 90 days of diagnosis. Respiratory copathogens were detected in 21 episodes (57%), including viruses (n = 12), fungi (n = 10), and bacteria (n = 8). Mortality rates were not different between patients with and without copathogens (P = .65). In multivariable models, mortality associated with HCoV LRTD was similar to that seen with RSV, influenza, and PIV LRTD in HCT recipients (adjusted hazard ratio, 1.34 [95% confidence interval, .66-2.71], P = .41 vs RSV, adjusted for cell source, cytopenia, copathogens, oxygen use, and steroid use).
CONCLUSIONS.: HCoV LRTD in patients with HCT or HM is associated with high rates of oxygen use and mortality. Mortality associated with HCoV LRTD in HCT recipients appears to be similar to that seen with RSV, influenza virus, and PIV.
人类冠状病毒(HCoV)在造血细胞移植(HCT)受者和血液系统恶性肿瘤(HM)患者的下呼吸道疾病(LRTD)中可能发挥的作用尚未得到充分研究。
我们对支气管肺泡灌洗(BAL)中检测到HCoV的HCT/HM患者进行了回顾性研究。使用菌株特异性聚合酶链反应在BAL样本中鉴定HCoV菌株。通过多变量Cox回归分析比较了由HCoV、呼吸道合胞病毒(RSV)、流感病毒或副流感病毒(PIV)引起的LRTD的HCT受者的死亡率。
我们鉴定出35例(37次发作)患有HCoV LRTD的患者。在23份可用的BAL样本中,48%为OC43菌株,22%为NL63菌株,17%为229E菌株,13%为HKU1菌株。总体而言,21例(60%)患者在诊断时需要吸氧治疗,19例(54%)在诊断后90天内死亡。在21次发作(57%)中检测到呼吸道合并病原体,包括病毒(n = 12)、真菌(n = 10)和细菌(n = 8)。有合并病原体和无合并病原体的患者死亡率无差异(P = 0.65)。在多变量模型中,HCT受者中与HCoV LRTD相关的死亡率与RSV、流感和PIV LRTD相似(调整后的风险比,1.34 [95%置信区间,0.66 - 2.71],与RSV相比P = 0.41,调整了细胞来源、血细胞减少、合并病原体、吸氧和使用类固醇)。
HCT或HM患者的HCoV LRTD与高吸氧率和死亡率相关。HCT受者中与HCoV LRTD相关的死亡率似乎与RSV、流感病毒和PIV相似。