Delaney Meghan, Stark Paul C, Suh Minhyung, Triulzi Darrell J, Hess John R, Steiner Marie E, Stowell Christopher P, Sloan Steven R
From the *Medical Division and Department of Laboratory Medicine, University of Washington, Seattle, Washington; †Center for Epidemiological and Statistical Research, New England Research Institutes (Data Coordinating Center), Watertown, Massachusetts; ‡Division of Transfusion Medicine, Department of Pathology, University of Pittsburgh, Pittsburgh, Pennsylvania; §Harborview Medical Center, Department of Laboratory Medicine and Division of Hematology, University of Washington, Seattle, Washington; ‖Department of Pediatrics, University of Minnesota, Minneapolis, Minnesota; ¶Department of Pathology, Massachusetts General Hospital, Harvard Medical School, Boston, Massachusetts; and #Department of Laboratory Medicine, Boston Children's Hospital and Department of Pathology, Harvard Medical School, Boston, Massachusetts.
Anesth Analg. 2017 Jun;124(6):1777-1782. doi: 10.1213/ANE.0000000000001926.
Cardiac surgery is the most common setting for massive transfusion in medically advanced countries. Studies of massive transfusion after injury suggest that the ratios of administered plasma and platelets (PLT) to red blood cells (RBCs) affect mortality. Data from the Red Cell Storage Duration Study (RECESS), a large randomized trial of the effect of RBC storage duration in patients undergoing complex cardiac surgery, were analyzed retrospectively to investigate the association between blood component ratios used in massively transfused patients and subsequent clinical outcomes.
Massive transfusion was defined as those who had ≥6 RBC units or ≥8 total blood components. For plasma, high ratio was defined as ≥1 plasma unit:1 RBC unit. For PLT transfusion, high ratio was defined as ≥0.2 PLT doses:1 RBC unit; PLT dose was defined as 1 apheresis PLT or 5 whole blood PLT equivalents. The clinical outcomes analyzed were mortality and the change in the Multiple Organ Dysfunction Score (ΔMODS) comparing the preoperative score with the highest composite score through the earliest of death, discharge, or day 7. Outcomes were compared between patients transfused with high and low ratios. Linear and Cox regression were used to explore relationships between predictors and continuous outcomes and time to event outcomes.
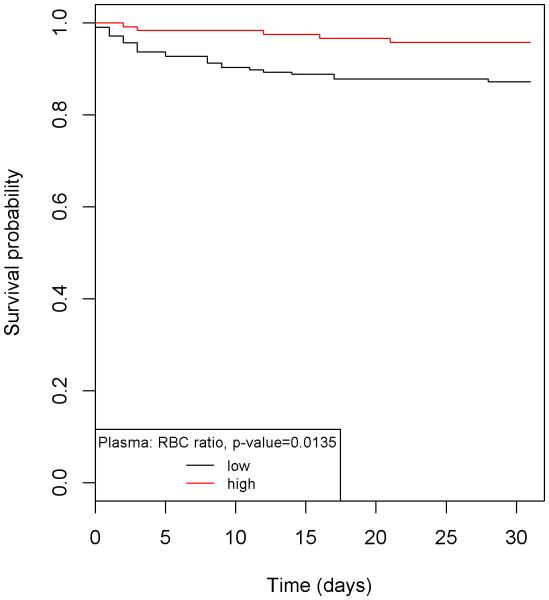
A total of 324 subjects met the definition of massive transfusion. In those receiving high plasma:RBC ratio, the mean (SE) 7- and 28-day ΔMODS was 1.24 (0.45) and 1.26 (0.56) points lower, (P = .007 and P = .024), respectively, than in patients receiving lower ratios. In patients receiving high PLT:RBC ratio, the mean (SE) 7- and 28-day ΔMODS were 1.55 (0.53) and 1.49 (0.65) points lower (P = .004 and P = .022), respectively. Subjects who received low-ratio plasma:RBC transfusion had excess 7-day mortality compared with those who received high ratio (7.2% vs 1.7%, respectively, P = .0318), which remained significant at 28 days (P = .035). The ratio of PLT:RBCs was not associated with differences in mortality.
This analysis found that in complex cardiac surgery patients who received massive transfusion, there was an association between the composition of blood products used and clinical outcomes. Specifically, there was less organ dysfunction in those who received high-ratio transfusions (plasma:RBCs and PLT:RBCs), and lower mortality in those who received high-ratio plasma:RBC transfusions.
在医学发达的国家,心脏手术是大量输血最常见的情况。创伤后大量输血的研究表明,输注的血浆和血小板(PLT)与红细胞(RBC)的比例会影响死亡率。对红细胞储存时间研究(RECESS)的数据进行回顾性分析,该研究是一项关于复杂心脏手术患者红细胞储存时间影响的大型随机试验,以调查大量输血患者使用的血液成分比例与后续临床结果之间的关联。
大量输血定义为输注≥6个红细胞单位或≥8个全血成分。对于血浆,高比例定义为≥1个血浆单位:1个红细胞单位。对于血小板输注,高比例定义为≥0.2个血小板剂量:1个红细胞单位;血小板剂量定义为1个单采血小板或5个全血血小板当量。分析的临床结果是死亡率以及多器官功能障碍评分的变化(ΔMODS),将术前评分与直至最早死亡、出院或第7天的最高综合评分进行比较。比较高比例和低比例输血患者的结果。使用线性回归和Cox回归来探索预测因素与连续结果以及事件发生时间结果之间的关系。
共有324名受试者符合大量输血的定义。在接受高血浆:红细胞比例的患者中,7天和28天的平均(SE)ΔMODS分别比接受低比例的患者低1.24(0.45)和1.26(0.56)分(P = 0.007和P = 0.024)。在接受高血小板:红细胞比例的患者中,7天和28天的平均(SE)ΔMODS分别低1.55(0.53)和1.49(0.65)分(P = 0.004和P = 0.022)。与接受高比例血浆:红细胞输血的患者相比,接受低比例血浆:红细胞输血的患者7天死亡率更高(分别为7.2%和1.7%,P = 0.0318),在28天时仍然显著(P = 0.035)。血小板:红细胞的比例与死亡率差异无关。
该分析发现,在接受大量输血的复杂心脏手术患者中,所使用的血液制品成分与临床结果之间存在关联。具体而言,接受高比例输血(血浆:红细胞和血小板:红细胞)的患者器官功能障碍较少,接受高比例血浆:红细胞输血的患者死亡率较低。