Rominski Sarah, Bell Sue Anne, Oduro George, Ampong Patience, Oteng Rockefeller, Donkor Peter
Global REACH, University of Michigan Medical School, Ann Arbor, MI 48103, United States.
Afr J Emerg Med. 2014 Jun;4(2):71-75. doi: 10.1016/j.afjem.2013.11.001. Epub 2014 Jan 17.
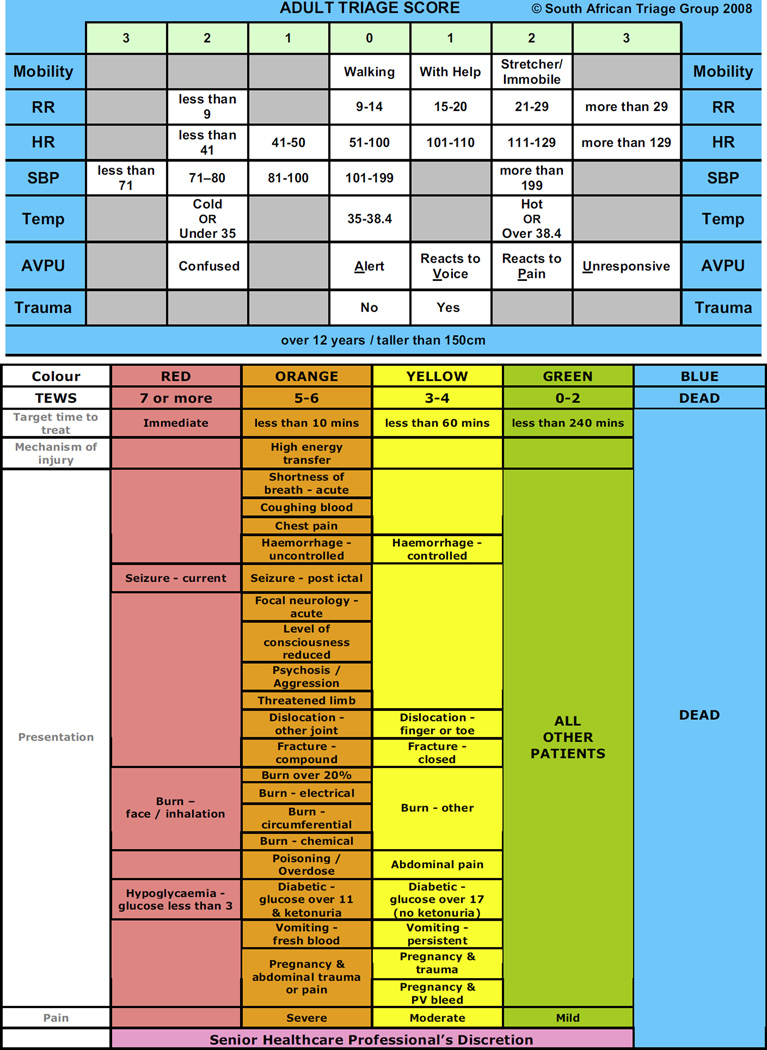
Triage is the process of sorting patients based on the level of acuity to ensure the most severely injured and ill patients receive timely care before their condition worsens. The South African Triage Scale (SATS) was developed out of a need for an accurate and objective measure of urgency based on physiological parameters and clinical discriminators that is easily implemented in low resource settings. SATS was introduced in the emergency center (EC) of Komfo Anokye Teaching Hospital (KATH) in January 2010. This study seeks to evaluate the accurate use of the SATS by nurses at KATH.
This cross-sectional study was conducted in the EC at KATH in Kumasi, Ghana. Patients 12 years and over with complete triage information were included in this study. Each component of SATS was calculated (i.e. for heart rate of 41-50, a score of 1 was given) and summed. This score was compared to the original triage score. When scores did not equate, the entire triage record was reviewed by an emergency physician and an advanced practice emergency nurse separately to determine if the triage was appropriate. These reviews were compared and consensus reached.
52 of 903 adult patients (5.8%) were judged to have been mis-triaged by expert review; 49 under-triaged (sent to a zone that corresponded to a lower acuity level than they should have been, based on their vital signs) and 3 over-triaged. Of the 49 patients who were under-triaged, 34 were under-triaged by one category and 7 by two categories.
Under-triage is a concern to patient care and safety, and while the under-triage rate of 5.7% in this sample falls within the 5-10% range considered unavoidable by the American College of Surgeons Committee on Trauma, concentrated efforts to regularly train triage nurses to ensure no patients are under-triaged have been undertaken. Overall though, SATS has been implemented successfully in the EC at KATH by triage nurses.
分诊是根据病情严重程度对患者进行分类的过程,以确保伤势最重和病情最危急的患者在病情恶化之前得到及时治疗。南非分诊量表(SATS)是基于生理参数和临床鉴别指标,为满足在资源匮乏环境中易于实施的准确、客观的紧急程度衡量需求而制定的。2010年1月,SATS在孔福·阿诺凯教学医院(KATH)的急诊科(EC)开始使用。本研究旨在评估KATH医院护士对SATS的准确使用情况。
本横断面研究在加纳库马西KATH医院的急诊科进行。本研究纳入了年龄在12岁及以上且有完整分诊信息的患者。计算SATS的每个组成部分(例如,心率为41 - 50时,得分为1分)并求和。将该分数与原始分诊分数进行比较。当分数不相等时,由一名急诊医生和一名高级急诊实践护士分别审查整个分诊记录,以确定分诊是否恰当。对这些审查结果进行比较并达成共识。
在903名成年患者中,有52名(5.8%)经专家审查被判定为分诊错误;49名分诊不足(根据生命体征,被送往了比其应属的病情严重程度更低的区域),3名分诊过度。在49名分诊不足的患者中,34名低了一个级别,7名低了两个级别。
分诊不足关乎患者护理和安全,虽然本样本中5.7%的分诊不足率处于美国外科医师学会创伤委员会认为不可避免的5 - 10%范围内,但已集中精力定期培训分诊护士,以确保没有患者被分诊不足。不过总体而言,SATS已被KATH医院急诊科的分诊护士成功应用。